
 Response to “Isabella B’s”
Response to “Isabella B’s”
“Why Dr Suzanne Humphries, an anti-vaccine activist, is lying to you about measles.”
by Suzanne Humphries, MD and Roman Bystrianyk
(This is also a response to our Amazon review by the same person who calls her/himself “Isabella B”.)
October 1st, 2015
| In this document, we have addressed every point that “Isabella B” made in her BLOG, in detail. See “Isabella B’s” critique in red, and the Dissolving Illusions’ authors’ responses in black. Two small sections of our response were intentionally duplicated in the text. |
Since this is the first negative review of our book that did more than just engage in a simple-minded, name-calling attack, we thought it would be important to respond to the points that were made.
Dr Humphries is not an “activist”. She is a conventionally educated doctor who used to prescribe vaccines and later saw vaccine damage occurring in her own patients. She was met with irrational resistance by hospital administration for cancelling vaccination orders in seriously sick patients with sepsis, congestive heart failure, acute kidney failure, cancer on chemotherapy etc. The hospital administrators required her to justify choices made for her own patients for the first time in her career. Because of this, she researched the medical literature on vaccination, only to discover that the words of those opposing her were built upon propagandized falsehoods.
Dr Suzanne Humphries, a nephrologist-turned-homeopath, is a prominent voice in the anti-vaccine movement. Her 2013 book “Dissolving Illustions”
Dr Humphries is a nephrologist and never has been a homeopath. Please see part one of this video for further explanation.
https://www.youtube.com/watch?v=cLrqmvjrIjI&list=PLgH2vCx5TOgX5upobA1NO–PyE60CLlVa&index=1
Mr. Bystrianyk and Dr Humphries did not write about “Illustions”. The book is called Dissolving Illusions: Disease, Vaccines and the Forgotten History.
was recommended to me by a homeopath when I had a baby and was unsure about the vaccine debate. However, the more I examined Dr Humphries’ claims and consulted the original studies she cited throughout her book, the more disappointed I became.
From what is written, it’s obvious that the book was not read thoroughly, since basic scientific and historical concepts are clearly missing in the critique.
Her claims are often misleading and at times outright deceptive.
No doctor resigns from a highly paid, very respectable job, then takes years out of her life, simply to deceive the public. Most of her critics will not even use their last names, or will use a totally made up pseudonym. Doing what Dr. Humphries did in leaving her job to speak publicly is tantamount to career and financial suicide. Clearly it was done for good reason.
Claim #1: Measles deaths are negligible
To start, Dr Humphries belabors the fact that measles deaths declined prior the introduction of the measles vaccine and implies that the vaccine was therefore unnecessary.
“Isabella B” has apparently missed one of the major purposes of the book. Dissolving Illusions discusses the overlooked and forgotten history regarding the horrible unhygienic conditions that people lived, labored and died under in the 1800s.
The key point made in the book is that the majority of infectious disease mortality declined across the board before the advent of vaccines, at the same time as other disease deaths declined; some diseases for which there was no vaccine at all.
Most of the credit for infectious disease mortality reduction, really goes to the radical moves over many decades to improve hygiene, sanitation, nutrition, implement water chlorination, labor laws, provide electricity, etc. Previously, society had endured constant plagues of one form or another. The spectacular reduction in infant mortality from 1800 to now in every developed country with careful records, has everything to do with societal
changes, and doctors learning to wash their hands. “Isabella B” either did not understand this point, or has no idea that the period of public health that we focused on – the mid 1800s to mid 1900s – did NOT include vaccines, antibiotics or even most pharmaceutical drugs that exist today. Or, she chose to ignore it.
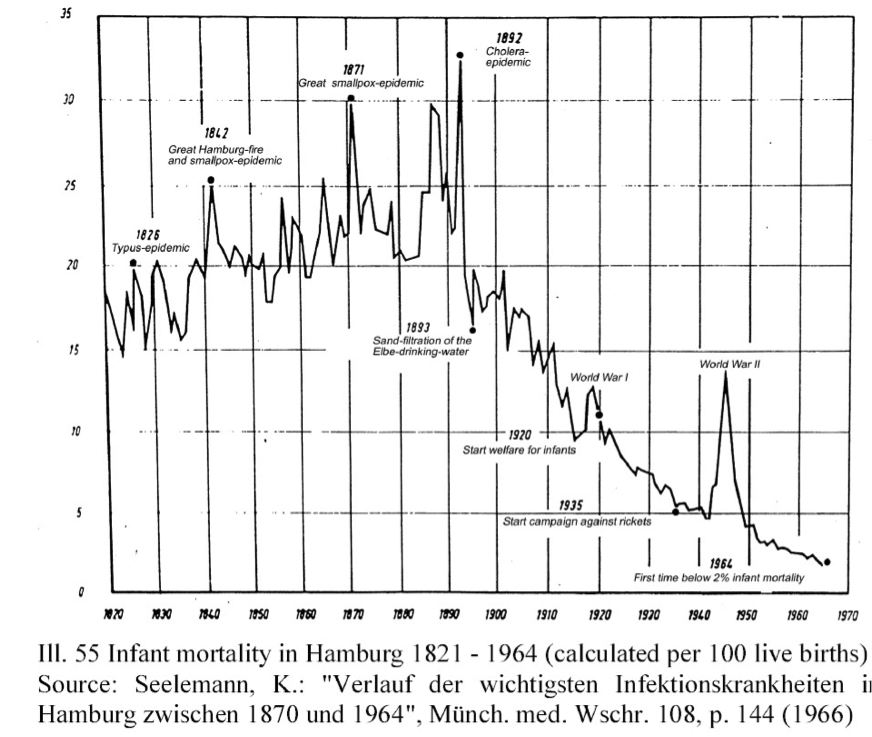
Everywhere in the developed world, Departments of Health hold Graphs like the one here from Hamburg, Germany, which very clearly shows the events which impacted most on the death rate.
“Isabella B” considers Dissolving Illusions’ concentration on death rate as “belaboring”, because it doesn’t suit her view of what is important.
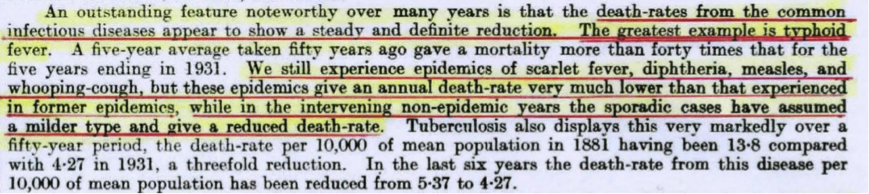
The fact is, that DEATH was THE most important indicator of societal “health” in history, until recently. Even smaller countries like New Zealand, had observant doctors who accurately reported what really matters. In the period we were writing about in Dissolving Illusions, the use of “death rates” was the primary indicator of progress, as evidenced by a report from the Director General of Health published in the Appendices to the (New Zealand) Parliamentary Journal, for the year 1932. In addition to talking about the decline in death, he mentions that the remaining diseases assumed a milder form, and thus a reduced complication and death rate.
When it came to Infant mortality the Director General had this to say:
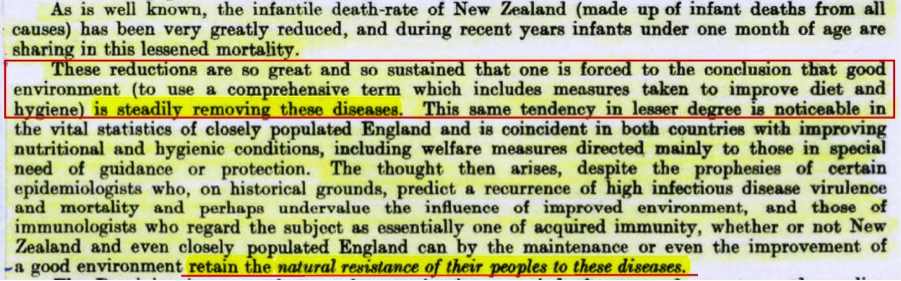
Note the words in the box above, and the underlining, that even though some diseases were “removed”, the epidemiologists of the time undervalued the effect of improved environment. It was his view from the data in front of him that the change in environment resulted in people acquiring an increased natural resistance to disease. The Director General of Health, who waded through the problems at ground zero, also pointed out that the same factors applied in other countries. He eloquently voiced the same dynamics as Dissolving Illusions does. The core issue today, is the same as it has always been: Resistance or susceptibility to disease is most positively influenced by fundamental principles of sound nutrition, clean water, sanitation, cleanliness and stress reduction, even in people who have immune system problems. The ability to kill germs with drugs, improve survival rates of car crashes with surgery, or prevent diseases with vaccines is secondary.
The 1946 Official Year book clearly shows the remarkable improvement in infant survival and health in New Zealand – all before any antibiotics came over the horizon:
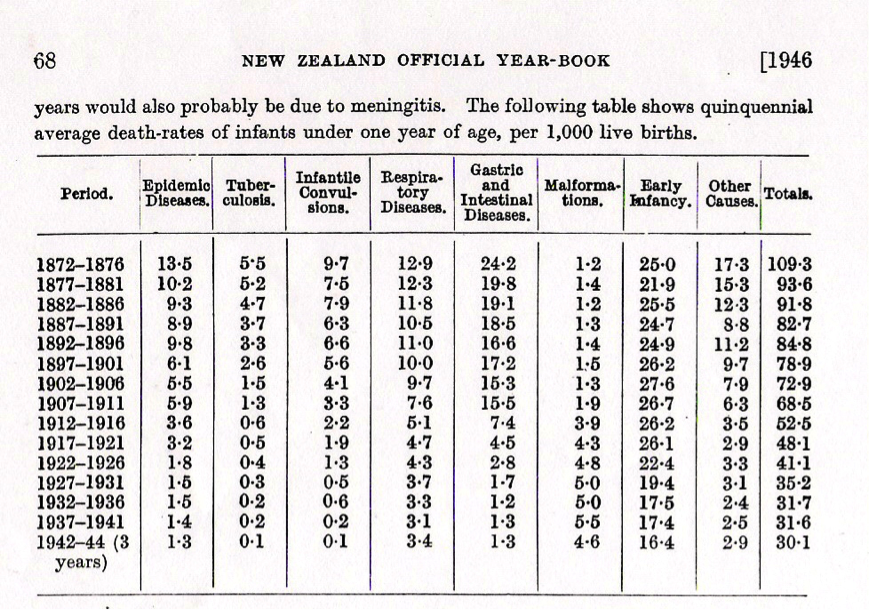
Death was, and is, one of the best, and most highly significant markers of overall societal health improvement. That is why all countries measured their progress by death decline, and increased lifespan.
That is why when doctors get angry if you won’t accept a vaccine, drug or test, they often say, “but your baby might die!” In 1994 when the UK was coerced into a mass vaccination campaign[1], it was the threat of death, not encephalopathy or blindness —that was used as the main tool to increase compliance.
Isn’t it fascinating how the landslide reduction in the very measure used to scare parents into vaccinating (death), is considered insignificant by “Isabella B”? Isn’t it interesting that interventions that so markedly reduced the death rate (hygiene and nutrition) get no or limited credit?
It is also noteworthy that Dr Peter Aaby wrote in 2012[2] that “The ultimate goal is to save lives, and vaccination programmes measure potential impact in terms of the lives saved.” Dissolving Illusions shows that the decline in death in the developed world had already occurred to the greatest extent, before vaccines for measles.
While measles case-fatality rates were indeed falling in high income countries like the US and UK from the 1900s until the 1960s due to improvements in living conditions and medical care, the disease incidence remained virtually unchanged until the introduction of the vaccine. In fact, almost everyone caught measles before the age of 15 at the time. The vaccine brought about a more than 90% reduction in disease incidence in a matter of a few years:
Yes, measles incidence did not decline significantly, in the way that incidence of diseases like tuberculosis, typhoid, scarlet fever etc, did as many of the 50 plus graphs made from public vital statistics show in Dissolving Illusions. Since “Isabella B” used measles as an example we will stick to that disease. This graph of USA incidence is really interesting. We have to take it at face value, but the question is, does it really portray what “Isabella B” says it does?
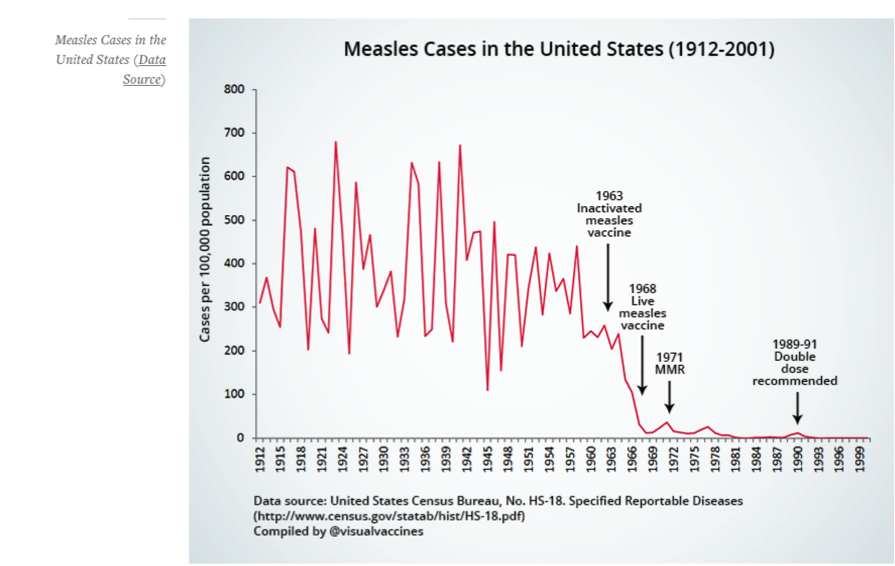
If you were to take your pen and draw out the peaks from 1912 to 1941 and then from 1941 to 1962 you would see that there is a decline in reported incidence.
In 1941 the case rate reached around 685 per 100,000. In 1962, the year before the vaccine was introduced, the reported case rate was 250 per 100,000.
That is a REPORTED 435 per 100,000 population case reduction in the 21 years before any measles vaccine was used in the USA. If there was no decline in incidence notifications at all, we would expect the peaks to have regularly remained around 700 but it never went anywhere near that for those years. Why might that be?
There are some other important key points which demonstrate that the vaccines used in the USA could not have been responsible for the case declines, and those points will be dealt with later.
This is another graph used by “Isabella B” showing England and Wales measles incidence rate:
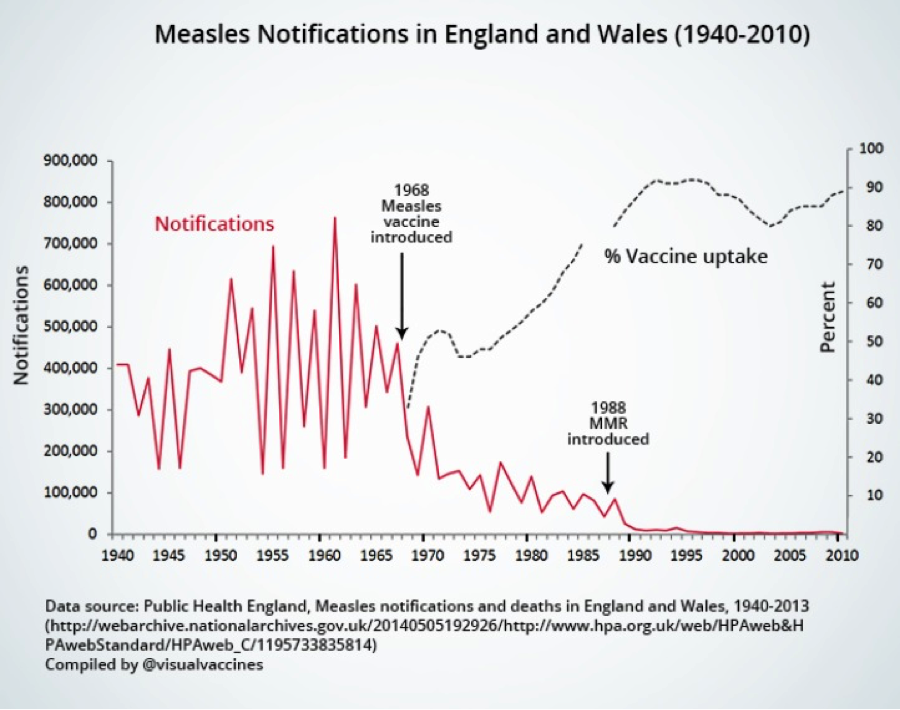
There was a decline in reported cases in the USA after the vaccine, and England and Wales…. but why? Some reasons are elaborated on later, but one reason could be that many people in the USA were becoming more comfortable with the disease and treating it at home just like parents and doctors in the UK were, as described in the BMJ in 1959.[3]
The 1950s medical literature stated by the attending doctors of the day that measles was generally considered a mild disease which doctors didn’t recommend trying to prevent. There was no inclination to prevent measles spreading, and children rarely needed any medical treatment at all. The infection was over in a week, and as BMJ published, the doctors said that many mothers remarked that their children were better for it afterwards. There were no special attempts made to prevent measles infections even in young infants in whom the disease has not been found to be especially serious.
So that was the prevailing medical attitude in 1959. What changed all that?
“Isabella B” is of the opinion that even though measles deaths were extremely rare, measles incidence did decline after 1963 so therefore “correlation most definitely equals causation”, and therefore the measles vaccine must be solely responsible.
The issue is more complicated than “Isabella B” appears to understand.
We explained this in Dissolving Illusions. In 1963, there were two measles vaccines. The first was the killed measles vaccine, which did not protect against measles. The recipients of that vaccine – when they came in contact with measles afterwards, got a much more serious form of measles; a susceptibility which the medical literature states lasted for up to 16 years[4].
At the same time, a non-attenuated live measles vaccine was used, which caused such severe side effects that it had to be administered with gammaglobulin to reduce the side effects and the severity of disease in the recipients. Anyone who got measles from this vaccine was not reported as having had measles.
So in the period between 1963 – 1968 one totally ineffective type of vaccine was used, which made recipients susceptible to a worse form of measles, and the other vaccine was a live, semi-attenuated one which “gave” people measles which was antidoted with gammaglobulin injected at the same time as the vaccine. Those were the ONLY two “vaccines” being used in the USA at the time that the so-called “landslide decline” in measles cases occurred.
The decline in reported cases can only be a statistical artifact similar to “observer bias”. In the years of the “landslide”, in the USA between 1963 and 1968, doctors simply got in first with the “vaccine” and created a blanket of “non wild-measles cases”, which they neutralized with gammaglobulin. These vaccine-induced cases took the place of wild measles transmission. Does that sound like a conspiracy or a reality? Look at the graph provided by “Isabella B” using data from the U.S. Census Bureau, Statistical Abstract of the United States: 2003, and then verify for yourself by reading pro-vaccine sites like this one http://www.historyofvaccines.org/content/timelines/all which describe which vaccines were available in those years in the USA. Then go and find out the effectiveness, danger and co-treatment that went hand in hand with those vaccines.
Today’s measles vaccines are further attenuated, but still have occasional problems related to symptoms and contagion. That is not conspiracy theory; that is well-published fact.
Quite apart from medically manipulated “non-measles”, in 1963, if a vaccinated person was infected and clinically symptomatic with measles, they would not be counted as having measles because they were vaccinated.
It is no different today. In California 2015, a child was counted as a measles case[5] until she got home to Alaska, whereupon, she was diagnosed as having vaccine-strain measles because of enhanced surveillance testing in the new outbreak. Because she had vaccine-strain measles, her case was then retracted from the measles count. A Canadian baby has also recently been struck from the record after her “measles” was found to be a vaccine-strain[6]. The number of “retracted” measles cases, world-wide is astonishing, and these are cases where children were diagnosed, often in a hospital, with “clinical” measles and the play centers or schools they attended were “sanitized” and all children and contacts revaccinated. Then we find out a few weeks later, that the case was “caused” by the MMR vaccine, and therefore removed from the statistics. Fortunately with the Internet, these cases often play out in the news and particularly on Facebook.
Mass vaccination can stop endemic disease outbreaks by removing wild virus transmission and circulation in the community, but does NOT induce permanent immunity in the vaccinated. It is well known and agreed upon, that because the measles vaccine gives a subclinical case of measles by injection, that the vaccine interrupted wild measles transmission. That is why we have low levels of wild measles today. The same applies to the oral poliovirus vaccine, which also carried enough risk so as to be discontinued in the USA.
What people like “Isabella B” ignore are the problems created by and inherent with vaccine control of disease. Vaccine immunity is not permanent, does not “improve” health, and does carry risk. Moreover there are benefits to recovery from measles disease, which Dissolving Illusions touches on, AND which was quite evident, even in the poorest sections of Africa[7]. The benefit that measles virus can bring is reflected by the fact that measles virus is actually used in high doses in attempt to treat certain cancers today. Since the regular vaccine does not produce the brisk immune response that a natural infection does, the cancer treatment has to use extremely high doses of vaccine measles virus for the desired effect. In the developed world today, where good nutrition is possible, where vitamin A is readily accessible just about everywhere, where knowledge about supporting a healthy immune system is available, there is no reason to have encephalitis of any sort, or for anyone to go blind with measles. Vaccine immunity is short-lived compared to normal infection with measles. Thus there is a valid argument against the vaccine measures undertaken from 1963 onwards that carried a promise of measles eradication with one shot to some children: A plan that looks ridiculous today to anyone who has all the facts.
Looking at rates of disease incidence — rather than mortality, as Dr Humphries does in her book — is important due to possible long term complications in survivors. Before the introduction of the measles vaccine in the US in the 1960s, for example, there were 4 000 cases of measles encephalitis a year (many of which led to irreversible neurological complications such as blindness, deafness and mental disability), 150 000 cases of respiratory complications a year, and 48 000 measles-related hospitalizations per year (which placed huge financial and emotional burdens on families).
As for complications in survivors, “Isabella B” is correct. This was a rare event in a small fraction of total cases; encephalitis, blindness or pneumonia, or the even rarer complication of Subacute Sclerosing Panencephalitis.
Wild measles-related encephalitis declined after the measles case-rate declined.
However, interestingly, the TOTAL all-cause encephalitis rates in countries that vaccinated and then bothered to look over a longer period of time, did not decline at all:
“The spectrum of encephalitis in children has changed due to vaccination programs. The incidence, however, appears to be about the same due to increasing frequency of other associated old and new microbes.”[8]
This is discussed in much greater detail below*.
If we consider that nutrition and living conditions were not very terribly different in the 1960s compared to today, and take an average of 500 measles deaths a year from that period, the measles vaccine possibly prevented up to 23 500 measles deaths from 1968 until 2014 in the US alone.
“Isabella B” cites 500 measles deaths per year, probably because she has heard that number from Paul Offit and others who are not held accountable for their words.
In the 10 years prior to the measles vaccine, there were an average of 440 deaths[9] per year, not 500.
But how is it that suddenly, the death rate became important to “Isabella B”, who initially berated the Dissolving Illusions authors for “belaboring” historical death decline before vaccination as a universal measuring rod?
If deaths are that important to “Isabella B”, then the interested reader is referred to the graphs, which show that the vaccine had nothing to do with the death rate declining for measles. Again . . . we find it amusing that the very interventions that reduced the death rate by over 98% (hygiene and nutrition) gets no credit in the view of the vaccine enthusiasts.
Furthermore, it is pity that Dr Humphries does not discuss at all the dramatic role the measles vaccine played in reducing infant mortality and blindness in developing nations in Africa and Asia.
Does “Isabella B” understand how measles causes blindness? It happens from a treatable condition called xeropthalmia, which leads to acute corneal ulceration in malnourished children who are deficient in a broad range of macro and micronutrients, particularly vitamin A. Xeropthalmia “is the commonest cause of childhood blindness in Northern Nigeria and usually develops after measles.”[10] This has been, and still is completely reversed by vitamin A treatment.[11] The author of this article states,
“Well-nourished children, however, only rarely develop complicated measles and they do not have bad corneal lesions… The clinical picture in malnourished measles patients is very typical and entirely similar to that of diseased children suffering from severe vitamin A deficiency i.e. xeropthalmia.”
This is why The World Health Organization (WHO) has regular vitamin A campaigns through the undeveloped world.
Ironically, two studies done in the USA[12], and one in New Zealand[13] show that children admitted to the hospital with measles are usually vitamin A deficient. The New Zealand study also identified other macro and micronutrient deficiencies as well, showing that nutritional knowledge poverty on the part of parents has a negative health impact on their children.
It is thoroughly documented in medical literature that well nourished children do not have the complication of blindness following measles.
It is a “pity” that Isabella does not understand the value of vitamin A and nutrition and the effects upon the morbidity of measles. If she did, she would know that while xeropthalmia is a problem in undernourished countries, it and other co-morbidities would be best remedied by food, rather than vaccinations with limited immune duration.
Nutrition and Vitamin A will be further expanded in point number 11.
Claim #2: Measles is a mild disease
Next, Dr Humphries claims that measles is at best a mild disease and nothing to fear. This may be true in many cases. However, as a homeopath, Dr Humphries may not be professionally inclined to see serious measles cases. As soon as measles complications do arise (eg such as coma or encephalitis) a sensible parent would rush their child off to hospital for treatment (which may involve antibiotics, an IV drip and a range of medical interventions to try and save the child’s life). If the child dies or develops complications in hospital such a hearing impairment or brain damage it is easy for the homeopath to retrospectively lay the blame for death or disability on “medical interventions”.
Again, repeating her false and divergent argument, “Isabella B” suggests that Dr. Humphries is a homeopath and that homeopaths do not see serious disease. (Which raises another question – why would “Isabella B” have taken advice from this homeopath?)
If “Isabella B” can produce any proof that Dr. Humphries practices homeopathy, this may be a point we would even bother to argue. However, given that Dr. Humphries is by training and experience, an Internal Medicine specialist, as well as a Nephrologist, both areas which mainly diagnose and treat worst-case scenarios, does “Isabella B” seriously believe that suddenly, over 20 years of clinical experience would have suddenly vaporized from Dr. Humphries’ memory?
Dr. Humphries also has a degree in Physics but the critics say she is not a physicist.
Dr. Humphries does NOT hold a homeopathy degree and does not practice homeopathy, but she is regularly called a homeopath and discredited solely upon that lie.
Dr. Humphries has a MD and a license to practice, and has taught medical students, residents, fellows and GPs in the topics of internal medicine and nephrology, yet that is regularly, conveniently ignored. This video series explains fully Dr. Humphries’ relationship with homeopathy.
https://www.youtube.com/watch?v=cLrqmvjrIjI&list=PLgH2vCx5TOgX5upobA1NO–PyE60CLlVa&index=1
Since homeopaths are by default not equipped to see life-threatening cases it is unfortunate when some presumptuously conclude that 1) measles is always a mild disease and that 2) when death or complications do occur, medical interventions are to “blame”. We should call this the “naturopaths-do-not-treat-serious-cases” fallacy:
Ask any physician who treated measles cases in the 1960s and they may paint a very different picture of the disease.
As previously stated, Dr. Humphries is more than well trained in seeing serious complications, and treating life threatening cases of everything as she regularly dealt with the sickest people in the tertiary care hospitals where she worked for two decades.
The fact is, that measles was MOSTLY a very mild disease in well-nourished populations where measles was endemic. Parents and physicians who dealt with measles in the 1950s knew it as a mild disease that was expected before age 15, and not something akin to the black plague or Ebola as today’s media and pro-vaccine dramatists would have you believe. This was reflected in television series’ of the early 1960s and in the older medical literature.
Dr. Alexander Langmuir, the father of modern day epidemiology was a strong supporter for development of the vaccine even though he knew that measles was a
“self-limiting infection of short duration, moderate severity, and low fatality, which has maintained a remarkable stable biological balance over the centuries.”[14]
He also stated,
“To those who ask me, ‘Why do you wish to eradicate measles?’ I reply with the same answer that [Sir Edmund] Hilary used when asked why he wished to climb Mt. Everest. He said ‘because it is there.’ To this may be added “And it can be done.”[15]
He never said, “Because it’s maiming thousands with blindness and encephalitis and killing hundreds, and is a blight worse than Black Plague”.
The CDC also reports[16] that before the vaccine only about 1/8th of all serologically measured positive cases ever was reported.
The Netherlands provides fascinating case studies on measles as it is a country with one of the highest living standards in the world, yet it has a “Bible Belt” that does not vaccinate. During a 2004/2005 measles outbreak with 3292 reported cases (94% of which were unvaccinated), 3 children died, 157 had to be hospitalized and 519 had complications (5 of which involved encephalitis). The study pointed out that “even in a wealthy country, measles is not just a mild childhood disease but can cause severe complications and even death.” The outbreak was unable to spread to areas with high vaccination coverage, indicating that these deaths and complications may have been avoided with sufficient vaccination coverage.
As in all measles outbreaks, that report showed there was a percentage of vaccinated patients with measles. Why is this? It is primary vaccine failure, secondary vaccine failure, or vaccine virus escape, which though rare, can happen.
The medical article states that the actual number of cases was between 23,000 and 37,000, not just the “reported” 3292 cases. Taking account of the true incidence rate of up to 37,000, takes the dramatic slant away, which is why “Isabella B” did not give all the facts related to the outbreak.
It’s obvious that most people stayed home and recovered uneventfully. Furthermore, the Netherlands outbreak cannot be compared to the pre-vaccine era at all. The Bible belt was essentially a virgin population where measles had not been circulating for decades, and therefore endemic exposure and regular waves of outbreaks were not the baseline. We know that measles affects virgin populations more seriously, than it affected the USA and UK in the 1950s.
One should also be aware that the 23,000 to 37,000 Dutch people who recovered will have solid, life-long immunity resulting in them being true contributors to herd immunity, as opposed to the vaccinated who will eventually jeopardize herd immunity as a result of primary and secondary vaccine failure[17], with their vaccine-induced immunity wearing off between 10 and 30 years later; a fact well published and mentioned in at least two peer reviewed articles.[18]
CLAIM #3: THE MEASLES VACCINE CAUSES ILLNESS.
She says, “A study from 1967 revealed that the vaccine could cause pneumonia as well as encephalopathy (p 347)”.
However, the 1967 study in question reviewed the inactivated measles vaccine (used on roughly 900,000 persons from 1963 until 1967) which was found to be ineffective and was replaced by the live measles vaccine from 1968 onward. The study has no bearing on the present-day immunization schedule. Numerous ramblings throughout this chapter on immune systems “wrongly programmed” by vaccines and committing “original antigenic sin” only relate to the inactivated (now defunct) measles vaccine.].
The killed vaccine is the ONLY vaccine discussed in pages 347 and 348. On page 366 – 369, antibody dependent enhancement and original antigenic sin is discussed in relation to the killed vaccine. Any other “ramblings”, are solely in the muddled mind of “Isabella B”.
“Isabella B” started out by saying we muddied the waters by talking about the 1963 vaccine and tried to deceive readers that that is the same vaccine used today.
Anyone who read the book with mental clarity would know that we were clear that the 1963-67 killed measles vaccine was just that… killed, and not the present day live vaccine.
Quite importantly “Isabella” admits that the killed measles virus vaccine use in 1963 was found to be ineffective. Yet, despite being ineffective the killed measles virus vaccine was somehow responsible for the majority of the “landslide” in decrease in measles cases.
Dr Humphries then claims that the live measles vaccine (introduced in 1968) was also ineffective and produced a rash in about half of those injected, but links to an archived source with the complete opposite title (which I was unable to locate), “Measles Vaccine Effective in Test — Injections with Live Virus Protect 100 Per Cent of Children in Epidemics,” New York Times, September 14, 1961.”
It took us about 30 seconds on Google to find both the article in the NY Times archives[19]
and the original NEJM article[20] which the NY Times referred to.
Here are the sections that were quoted in Dissolving Illusions.

As is well known in any of today’s papers, you can have a title of an article, but the body tells another story. In this case it was that the vaccines produced a “modified measles” rash in about half of those injected—essentially equivalent to a case of measles. Forty-eight percent of people had rash, and 83 percent had fevers up to 106°F post-injection. To temper this problem, measles-specific antibody was given in the form of immune serum globulin alongside the live vaccines. This is explicitly stated in both references cited that “Isabella B” could not find.
It is well known that the live measles vaccine can lead to a mild rash and fever a few weeks after immunization, as the body reacts to the live attenuated (weakened) virus. This does not, however, mean that the measles vaccine “failed” — as Dr Humphries seems to imply above — but rather that the body is forming an appropriate and successful immune response to the attenuated virus.
Anyone who has read the chapter section where the safety record of measles vaccines was discussed will attest that we never said the vaccine failed because it created a rash and fever of 106 degrees. We said that the vaccine essentially gives a person a time-chosen, case of injected measles, and then afterwards, this is not called a “case”.
If “Isabella B” had taken the time to understand the history of measles, she would know that the original stated intention of the measles vaccine deployment was to ERADICATE measles by 1967[21] with a one-shot program to just part of the childhood population. Contrast that to today where we are seeing measles in babies because their mothers are vaccinated and not naturally immune, seeing measles in teens and adults because of waning immunity from their TWO dose regimen and what Peter Aaby says in 2003:
“The greatest threat to eradication might be waning immunity among vaccinated persons, resulting in secondary vaccine failure and low vaccine efficacy.” [22]
Which of course means lifelong vaccines for all of us in the future. And if you think measles vaccines will ever stop even after eradication, think again. Now they say 1) The vaccine is so beneficial that we need it whether measles exists or not. This is based on reductionist junk science and no gold standard trials. The fact is that measles disease itself gives lifelong immunity and all the benefits of vaccination without the need for continuous injections of laboratory manufactured vaccines. 2) That virgin soil populations are sitting ducks for bioterrorism so we all need measles vaccines forever.
It should be obvious to anyone that the measles vaccine program did ultimately fail in its original stated goal, even if it interrupted wild virus transmission to a large degree. Imported cases will remain problematic even with 100% vaccine uptake rates. And after the naturally immune members of the population die off, the problem will become even bigger, as we are beginning to see today.
The reason the public accepted this vaccine was the promise of measles eradication by 1967 with a one-shot program. That is a deal that most people would have signed onto in 1967. But it turned out that it was just the start, when it came to the number of measles injections ultimately needed to supposedly eradicate measles.
Today with two measles vaccines to over 95% of the USA children and repeat vaccines later in life, we are left with:
- Vaccinated mothers who do not protect their young infants like naturally immune mothers did, and thus a MORE vulnerable infant population.[23]
- A number of susceptibles in highly vaccinated populations that far exceeds the number of adolescent and adult susceptibles in the pre-vaccine era.
Why? Because of primary and secondary vaccine failure; something that prominent vaccinologists write about.[24]
This year, the media has used hyped-up propaganda, portraying measles illness as worse than Ebola or the black plague.

Today the measles outbreaks in the USA are blamed on the vaccine refusers, despite the fact that half of the cases from the California Disneyland outbreak were of “unknown” vaccination status and 18% were fully vaccinated[25].
After people who have immunity from the natural measles pass away, we will be seeing more than 18% vaccinated in future outbreaks. At least two medical articles predict that. So yes, the original stated goal of the measles vaccine failed.
In a few more years this will become even more painfully obvious as more and more MMR booster shots will be added to the schedule, and could be mandated for us all.
Bizarrely, she alleges that this post-vaccine measles rash should in fact be counted as genuine measles to boost the number of annual notifications and prove that the vaccine is ineffective:
Given that at least 5–10% of measles vaccine result in fever and rash, then there are approx. 650,000–1,300,000 case of measles in the US per year (p 372).
Shouldn’t a full blown case of mumps after the mumps vaccine, also be counted as a case of mumps?
If a person gets chickenpox after the chickenpox vaccine, that is counted as chickenpox.
CDC says to clinically treat vaccine-strain cases just the same as wild cases.
Is it not BIZARRE that the medical system treats chickenpox after a vaccine, as a case, but not measles after the measles vaccine?
It’s not a matter of “boosting annual notifications”. It’s a matter of accurate reporting. What we have now is disguised data.
For measles cases to be in the statistics, they must fulfill certain criteria that are outlined by CDC and repeated in Dissolving Illusions.
No serologic evidence is required if you are symptomatic and linked to a confirmed WILD-measles case.
In the absence of heightened surveillance, if you are diagnosed with measles and were vaccinated within 18 days, genetic testing is done to distinguish vaccine strain infections and if your measles is caused by the vaccine strain, that isn’t considered measles. Is that not bizarre?
The existence of measles infection in children who are infected by the vaccine virus should be counted as measles. Why? Because we know that vaccine-strain infections occur beyond 18 days of vaccination[26].
In the USA this year, two cases of measles were diagnosed on clinical grounds but when the virus was genetically sequenced and shown to be the vaccine strain virus, those cases were struck from the record.
Do you think that is science?
Do you think that is honest record keeping?
One of them was considered to have picked up the virus from daycare from another vaccinated child.[27]
What follows is a lengthy discussion on how “incomplete clearance of measles virus and deranged immune responses have a known association with chronic clinical and subclinical infection” (p 350).
The discussion of how incomplete clearance of measles virus has an association with chronic and subclinical infection referenced the Uhlmann 2002 paper, and was not a ‘mistaken belief about any 1963 inactivated virus’ as she insinuates below.
This is based on the mistaken belief (possibly drawing conclusions from the 1963 inactivated measles vaccine) that the measles virus elicits an antibody-only immune response. The reality, however, is that the live measles vaccine elicits both an antibody mediated and cell-mediated immune response. This is discussed in more detail below with citations.
The rest of this section contains the following supporting citations:
a) A paper by the discredited Dr Wakefield which has been thoroughly debunked elsewhere
b) The famous Lancet paper by Dr Wakefield which was retracted due to concerns about fraud and falsification
c) A paper on delayed reflexes in newborn primates who received the thimerosal-containing Hep B vaccine, a questionable study funded by anti-vaccine activists which too has been debunked
d) Papers by Dr Stephen Walker that supposedly support Dr Wakefield’s autism claims.
However, this is what Dr Stephen Walker has repeatedly said of his own studies:
Some observers have said that the presence of the measles virus indicates a strong possibility that the measles vaccine, a possible source of the virus, could have caused the children’s autism. […] Walker says the new research does not support the connection, and he notes that the results have not even been published in a peer-reviewed journal. “Even if we showed association (between measles virus and bowel disease) and we published it in a peer-reviewed journal, the conclusion will be simply that there is measles virus in the gut of a large number of children who have regressive autism and bowel disease. End of story.
We haven’t done anything to demonstrate that the measles virus is causing autism or even causing bowel disease.
We were criticized for our sources when describing neurologically impaired children and the association to the MMR vaccine and vaccine virus in their tissues.
“Isabella B” said we used Dr. Wakefield’s Lancet papers as supporting citations.
We did not use them as supporting citations, or to make conclusions at all.
They were specifically listed as a historical description of studies that were retracted or removed.
Dr. Walker’s poster presentation clearly found vaccine-strain virus in the bowel lesions of autistic children. Whatever he later said does not negate the words that his own fingers typed into his poster findings.
| Dr Walker stated to Dr. Humphries directly in a personal email on December 28th, 2012 the following: “Because I specifically wanted to know if the MV [Measles Virus] fragments found in the ileocolonic tissue were of vaccine strain origin, I made PCR primers designed to generate an amplicon that included a base pair that could serve to distinguish WT from vaccine-strain MV. Our preliminary results, presented at the IMFAR in Montreal in 2006, were very supportive of that thesis. I have attached the poster, as you requested. . . . I haven’t done anything more on it for quite a while, although now I have plenty of samples. Funding to complete the work was/is one issue. The other is the publicity aspect.” |
Dr Walker’s conclusions and public statements were used by “Isabella B” in order to downplay his findings of vaccine strain virus in autistic children with bowel disease.
“Isabella B” made an attempt to diminish Dr Walker’s work, by quoting public statements made after he was hounded by the pro and anti-vaccine.
He never stepped away from his findings in any of his statements and the above message to me, reveals what he found, why he could not continue, and what his concerns were.
“End of story?” Far from it. This is a case of story interruptus, due to funds drying up, which was also the reason Dr. VK Singh could not continue his work.
If you have not heard of Dr. VK Singh, his published medical studies[28] showed that autistic children compared to normal controls had enormously elevated anti-MMR vaccine antibody, anti-MV antibody, and antibodies against parts of the brain such as Anti-Caudate nucleus antibody, Anti-cerebellum antibody and markedly elevated anti-myelin basic protein antibody.
Dr. Singh made a plea to Congress in the year 2000 for funding to help the many autistic children who had these brain symptoms as a result of over reactivity towards the MMR vaccine. The result of his public request for money to continue his research was the drying up of his funds.
“This was most probably the first laboratory-based evidence to link measles virus and/or MMR vaccine to autoimmunity in children with autism. Collectively, these observations led me to speculate that autism may be caused by a measles or MMR vaccine-induced autoimmune response.
Unfortunately, due to lack of funding, I have not been able to extend this research and the progress has been hampered.”[29]
What followed were the fatally flawed studies done by CDC and Danish scientists, which supposedly debunked any connection between autism, brain damage, and the MMR vaccine. One of the lead researchers of the thimerosal-autism work recently had a pang of conscience and came forward to tell of the unethical and fraudulent data manipulation that he saw occurring in the 2004 study.
It remains to be seen what Dr Thompson will do next.
After Thompson’s confession to cooking the data books with the other scientists to bury over a 236% increased risk of autism in black children in the 2004 paper, Paul Offit described Dr. Thomson as having “psychological problems”.[30]
That’s pretty typical. Any scientist who dares to discuss science which questions the “vaccines are safe, effective and necessary and the science shows that” mantra is branded a quack, a fraud, psychologically unstable, a homeopath, or funded by the anti-vaccine movement.
Apparently to be credible, you have to quote only cherry-picked approved studies, and be funded by the manufacturer of vaccines, or occupy a university chair position funded by Merck.
No problematic associations there, right? To suggest as much could make us “conspiracy theorists”.
Claim #4: The measles vaccine can be crippling or deadly
Dr Humphries then reveals that “the vaccine has essentially induced cases of measles that were either benign, crippling or deadly” (p. 354) but fails to provide the context for these claims.
Incorrect. The context is right there in the references in the bottom of the page and the next page:
For the word “crippling” she cites a study that examined encephalopathy as an incredibly rare complication of the vaccine — 48 temporally related cases out of 75 million children. In fact, the study outlines various caveats and emphasises the rarity of the phenomenon:
It is a fact that the measles vaccine can be crippling or deadly. No parent can be guaranteed a risk-free vaccine. No placebo-controlled safety study has EVER been done on humans for the MMR vaccine looking for neurological and autoimmune outcomes in the short and long terms. The earliest vaccine tables for injury compensation listed and allowed MMR claims for hematologic, neurologic and autoimmune disease damage. The USA’s health authorities and lawmakers agreed there was danger with the vaccine. Within two years, there were so many demands on the public taxpayer’s money to compensate MMR victims that the lists on later tables were radically narrowed down. Dr. J A Morris, who was a vaccine safety scientist at the FDA in those days, has written and spoken that this was not a medical decision, but a financial one.[31]
Add to that the fact that vaccine-strain measles is frequently found in symptomatic children.
Why do we not hear about this more often? Because the technology to distinguish between vaccine strain and wild measles was not commonly available until relatively recently AND because as Kaic[32] and Murti[33] have well documented only during heightened surveillance is the virus genotyped at all.
We are told we must protect cancer patients by making sure everyone around them is vaccinated. But how often is vaccine-strain measles contagious to cancer patients? We don’t know because nobody tests. But, if you are a cancer patient undergoing treatment you and your family will be given a document telling you, that none of your family or friends should be allowed to come near you if they have had ANY live viral vaccines such as chicken pox, measles, rubella, inhaled influenza, oral polio, rotavirus or smallpox vaccines.[34] So plainly, vaccines can cripple, and it can’t be that rare.
The argument of vaccinating to protect cancer patients, is then extended to all persons with an immunodeficiency or a chemically suppressed immune system, on the basis that they have the right to go wherever they want with no restrictions. Apparently there is no concern about the myriad of other equally dangerous infections that could topple them, for which there are no vaccines.
As for showing that measles vaccine can cause harm, all one has to do is look up the VAERS database to see damage and death. Cases have been settled worldwide for MMR vaccine-damaged children (including autism). It is not a matter of opinion that the measles portion can cause severe or mild damage. It is a matter of verifiable fact.
From 1970 to 1993 in the United States, approximately 75 000 000 children received measles vaccine by age 4 years based on 83 000 000 births over 23 years and an immunization rate of 90%. The 48 cases of encephalopathy probably represent underreporting to this passive system, which does not require individuals to file for compensation and requires medical documentation.
However, given the generous compensation offered in this program, it is reasonable to conclude that most serious cases temporally related to a vaccination have been captured. In the absence of a specific test to determine vaccine causation, these 48 cases may include some nonvaccine cases representing background rates. Nevertheless, with a denominator of 75 000 000 vaccinees throughout 23 years, the incidence of acute encephalopathy caused by measles vaccine in this cohort can reasonably be decreased as very low.
In short, even if all cases were indeed proven to be causally linked to the vaccine, the risk of developing encephalopathy from the vaccine would amount to 48/75 000 000 or 0.00006%, and is typically related to underlying immune related disorders. Dr Humphries does not mention these figures and fails to discuss the risks of developing encephalopathy from the wild form of measles, which remains 1 out of 1000 cases or 0.1% in developed countries (higher in developing nations) and presents in otherwise healthy individuals.
The above study by Weibel is used in Dissolving Illusions ONLY as an example that the vaccine “can be crippling”: not that the study represented a comprehensive total of all vaccine injuries.
Weibel looked at 48 cases that fit the inclusion criteria and that presented to doctors between 1970 and 1993. Here were the criteria for inclusion in the study.
“Children with appropriate development who acquired an acute encephalopathy of undetermined cause within 15 days after the administration of the first dose of measles, MR, MMR, mumps, or rubella vaccine between April 1970 and March 1993 followed by chronic encephalopathy or death were selected for further analysis. . . Cases of encephalopathy were excluded if an infectious, toxic, traumatic, or metabolic cause or a recent exposure to natural measles, mumps, or rubella was identified or full recovery occurred within 6 months.”
Many of these cases were gathered from CDC reports or legal documents.
We did not use this study in Dissolving Illusions as an example of the huge volume of brain injuries post-vaccine, but rather as an example that crippling can occur and the conclusion of Weibel’s paper is that there is a relationship.
“Isabella B” used the Weibel paper as an example that encephalopathy is extremely rare. Here is why this paper should not be used in that way:
A good mechanism for quantification of cases is absent from Weibel’s study. Why? Because there was no reporting system in place between 1970 and 1988. Reporting was passive. Not all of the cases that occurred prior to 1988’s Vaccine Injury Compensation Program were reported through the 8-year retroactive policy. From 1970 to 1980 there was no encouragement to report at all. Even today in the era of increased awareness of vaccine injury and VAERS, many parents and doctors never make the connection between serious neurological disease and vaccines.
Once VAERS was in place, there was a window of reporting of MMR vaccine encephalopathy occurring up to 15 days of onset of illness that persisted for greater than 6 months. Anyone who fit these criteria and knew they could report it could apply to try to get compensation.
In reality, encephalopathy doesn’t occur within the bounds of table limits. What happens if encephalopathy occurs on day 16, and/or resolved in five months and 3 weeks? Who paid the medical bills if recovery was before six months? The Vaccine injury table is only applicable to a minority of the most serious cases, so long as they conform to a legal time frame, which is much shorter than encephalopathy following the vaccine, as specified in Merck’s MMRII datasheet.
The study by Weibel can only be used as an example – as they conclude, that a “causal relationship between measles vaccine and encephalopathy may exist as a rare complication of measles immunization.” Weibel’s study is a huge underestimation of actual cases, because of the lack of reporting systems, knowledge of such systems, and the limitations of the system for compensation.
Secondly “Isabella B” used what amounts to a theoretical calculation from Weibel himself to assume that vaccine related encephalitis is very rare. Here is why the numbers in the calculation are mostly theoretical: There is no evidence of a vaccine uptake rate of 90% between 1970 and 1993 and in fact evidence exists that the uptake was much lower in those earlier years. The only number that can be verified is the 83 million live births. The 48 cases could be a gross underestimation and the 90% vaccine uptake is a gross overestimation. Thus the conclusions that measles encephalopathy after MMR must therefore be very rare, is unfounded by the paper and not the main intention of the authors use of the paper anyway.
Encephalitis is not the only serious potential adverse outcome of the MMR vaccine. Immune Thrombocytopenic Purpura can be a serious outcome of MMR vaccination. Most medical reports state it is a benign entity, however the treatment can range from observation to steroids to IVIG to IV RhIG. The reported risk is approximately 1 in 24,000[35] to 30,000[36] to 40,000[37] vaccinees.
Other potential adverse outcomes exist; deafness, long-term seizures, coma, lowered consciousness, and permanent brain damage. How often? No-one can say for sure but the magic number of one in a million is often mentioned. What is the risk for any adverse outcome? It is hard to tell since data are inadequate. According to a recent Cochrane study, “The design and reporting of safety outcomes in MMR vaccine studies, both pre- and post-marketing, are largely inadequate.”[38]
For the word “deadly” she cites a study that examined the unfortunate case of a boy who died 8.5 months after the MMR vaccine. However, the study revealed severe immunodeficiency in the patient which would normally be diagnosed before 9 months of age and lead to medical exemption from vaccines with live viruses. His case was therefore extremely unusual and unfortunate:
In the case above, of the boy who died 8.5 months after the MMR vaccine, it should be the job of a physician to consider that constant infections could indicate that there MIGHT be an immune deficiency and test for it, BEFORE a vaccine is given, but it is not true that these cases are normally diagnosed before 9 months. Dr Humphries was consulted by a mother whose child was constantly on antibiotics, vaccinated and 20 months old. The doctors wanted to give MMR and were hounding her. Dr Humphries suggested that the baby should be tested for immune deficiency and sure enough, the tests returned as a selective IgM deficiency.
If encephalopathy from wild measles “presents in otherwise healthy individuals” (as “Isabella B” states above) then technically the total number of encephalopathy cases should fall after a successful vaccination campaign.
As many case histories prove, victims of infectious encephalopathy usually have an immune system defect, which leaves them susceptible to any pathogen that has this potential.
As for encephalopathy in a minority of children infected with wild measles, “Isabella B” is correct. This was a rare event in the era of wild measles. It is also true that specific wild measles-related encephalitis did decline after the vaccine interrupted wild measles in countries that vaccinated heavily. But the bigger picture shows a pattern that should be noted.
*In his earlier report[39], Koskiniemi said that total encephalitis cases declined, as seen in this table which looks at the years 1968 – 1987. The nationwide MMR campaign began in 1982 with an 85% uptake.
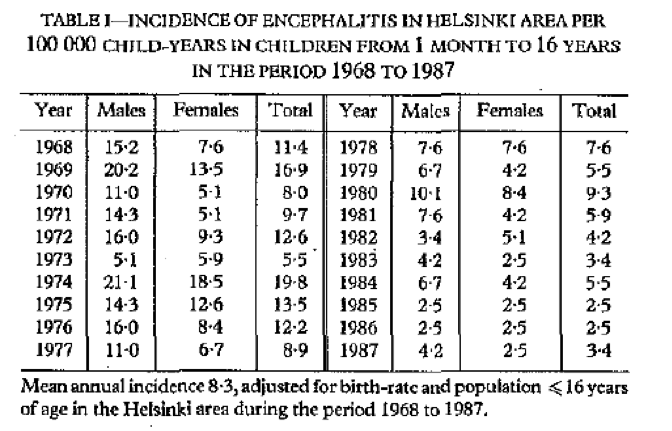
Dr Koskiniemi noted that while the total cases declined (as you can see when taking the average before which is 10.4 and after the vaccine which is 3.6), the severity had actually increased.
“The eradicative effect of MMR vaccination, confirmed in the Helsinki area, is gratifying. Unfortunately, the decrease in the number of encephalitides has not been accompanied by a decrease in the proportion of severe cases. . . . Although the number of all cases per year has fallen considerably, the number of severe cases has remained static despite the high rates in 1973-77. Thus the proportion of severe cases has increased.”[emphasis ours][40]
Here is the table showing the increase from 7.2% average pre vaccine to 17.1% post vaccine

In the initial 1989 report Koskiniemi said:
“The incidence of 8/100,000 with a peak of 20/100,000 in 1974 resembles that reported by others, though a decrease was evident over the study period.”
In the later 1997 report[41], Koskiniemi noted a rate of 10.2 per 100,000 total cases in the two-year period from January 1993- December1994, which is not much of a decrease at all. While early reports immediately after the vaccine looked promising, later numbers revealed that total encephalitis rates had not changed much at all.
“The spectrum of encephalitis in children has changed due to vaccination programs. The incidence, however, appears to be about the same due to increasing frequency of other associated old and new microbes.”[42]
And this makes total sense, because if a child has a defect in cell mediated immunity from any cause, they are sitting ducks to be picked off by other microbes such as VZV, respiratory, enteroviruses, Chlamydia, HHV-6, or any of the 20 different organisms found in Koskiniemi’s series of cases.
Yet the reductionist scientists and statisticians of the rabidly pro-vaccine camp will simply gaze into the tunnel-vision-looking-glass and point out that measles cases went down, and measles-related encephalitis declined. As always, and as we point out over and over in Dissolving Illusions, the bigger picture over the longer term is what should be analyzed, when evaluating any vaccine program.
We believe that the present report is the first to clearly demonstrate that severe neurological disease can be caused by the vaccine strain of measles virus. The risk of such a serious adverse event must be balanced by the rarity of such an event and the overwhelming evidence supporting the efficacy of the vaccine in reducing the morbidity and mortality associated with measles. It is significant that our patient was found to suffer from a profound deficiency of CD8 cells as well as dysgammaglobulinemia, which were not suspected clinically at the time of vaccination.
Most significant primary immunodeficiency states in children will be detected before the age of MMR vaccination, and for such children live virus vaccines should be avoided.
Here is the history of the child before they diagnosed the so-called immune deficiency.
“We report a case of measles inclusion-body encephalitis (MIBE) occurring in an apparently healthy 21-month-old boy 8.5 months after measles-mumps-rubella vaccination. He had no prior evidence of immune deficiency and no history of measles exposure or clinical disease.”[43]
The article says something else that “Isabella B” naturally ignored:
“An immunologic evaluation of this patient was prompted by the diagnosis of MIBE. While we cannot ascribe his condition to any classic immunodeficiency syndrome, our findings support the presence of a primary immunodeficiency. Most significantly, a profoundly depressed CD8 cell population was demonstrated.”
A thorough evaluation turned up NO classic immunodeficiency syndrome.
The parents of that boy must be disappointed that their son’s immunodeficiency was not considered or diagnosed and discovered before the vaccine. How was it explained to them? Would knowing that “most significant primary immunodeficiency states in children are detected before the age of MMR vaccination” be comforting to parents grieving over their dead child? Were they told that this was a potential outcome? Would he have lived the rest of his life normally if he had not been vaccinated? Can the parents be assured the profoundly depressed CD8 cell population was not related to previous vaccines?
Clearly, a serious outcome such as occurred for this patient is an exceedingly rare event, and this report should not lead to changes in current immunization practices.
Parents should be made aware of such a potential outcome. Doctors should be observant enough to diagnose the obvious… but often, they are not. Doctors consider it normal to prescribe numerous courses of antibiotics to infants and toddlers, so what would prompt the doctor to look at the underlying reasons for these infections. When do doctors look for immunodeficiencies?
Since the wild form of measles leads to much higher complication and death rates even in high income nations, it is unclear exactly what Dr Humphries is suggesting as the alternative here. Unless a parent can successfully “hide in the herd” and guarantee that one’s child will never be exposed to measles during the entire course of his or her life, the risks of death and encephalopathy from the wild form of measles are statistically thousands of times greater than that of the vaccine.
This is an assumption on “Isabella B’s” part, and would only apply to the tiny minority of people who are at risk of encephalitis complications. For 99.99% of healthy children the chances of encephalitis and death from measles is always ZERO. History proves that. We have no well designed study to back up her statistical risk statement, mostly because the incidence of measles pre-vaccine has been grossly underestimated in the official reports. Also, there is no data available on the incidence of SSPE prior to 1970.[44] Such data is important. Knowing the SSPE rates in the 1950s pre-vaccine, and then how they might have been affected during the killed and poorly attenuated measles campaigns in the 1960s would indeed be interesting.
Furthermore, if it is true that total encephalopathy rates don’t change because other pathogens step into measles’ place and fill the gap, thereby taking advantage of an immune system susceptibility of that child/person, then the only way to protect such a child is to magically remove from their world, the many pathogens for which there are no vaccines, that can also cause encephalitis or death.
CLAIM #5: MEASLES VACCINATION DOES NOT PROTECT AGAINST ALL STRAINS
On page 355 Dr Humphries claims:
Thirteen million doses of measles vaccine are injected each year. Those live viruses are attenuated, and the strains will vary from time to time in the manufacturing process, which means that immunity to one strain does not necessarily confer immunity to wild virus or to future virus.
This is incorrect. While there are 19 genotypes of measles, there is only one serotype. In other words, antibodies against one genotype will protect against all other genotypes, which is why measles immunity is typically considered lifelong. The following explanatory graph was kindly put together by an immunologist at Vaccine Nation:
http://www.vidrl.org.au/laboratories/measles-reference/measles-virus-genotypes/
First the genotype issue:
The Genotypes that “Isabella B” mentioned is incorrect:
We have always been told that measles is a single serotype virus, meaning that its surface antigens are pretty well conserved even though it is an RNA virus, which usually tend to be quite unstable on a genetic level. Since the use of PCR, eight clades or branches of the measles virus family tree have been defined, and 24 genotypes[45], NOT 19 as “Isabella B” stated, where in a fit of inattention, “she” used a blogger’s reference.
Now to the rest:
In general and in the past, the assumption has been that the vaccine virus does and always will, cover all strains.
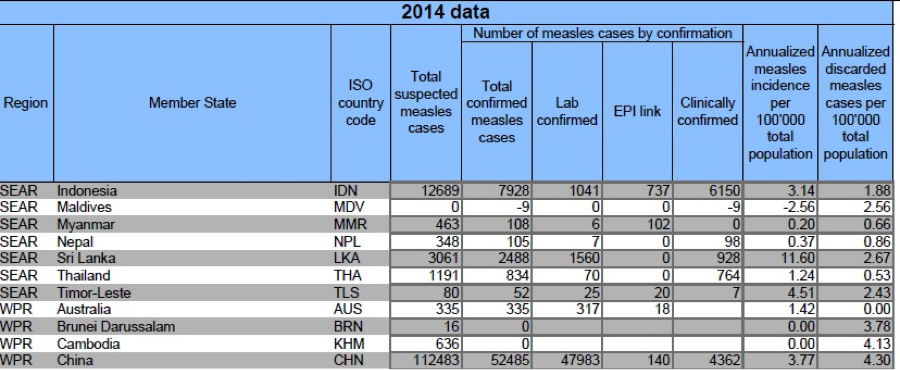
However, this doesn’t explain the WHO’s reported high rates of measles in some countries with very high vaccination rate, such as China’s which has a 99% vaccine uptake[46].
The theory is that vaccine immunity covers everything, and that China is so big, and crowded that that explains their high numbers of measles. But if that is true then how can the strains described in Finsterbusch[47] have evaded the vaccine-induced antibodies in laboratory tests? The “explanation” in the article is that certain strains aren’t recognized by measles antibodies derived from vaccines, but they also contradicted themselves by saying that they were still effectively neutralized by vaccine-induced polyclonal human sera.
But then they go on to say “The implications of the [mutant] L397 variant are not easy to assess, but results obtained for other viruses point at a certain risk potential regarding escape from antibodies provided by vaccination or previous infection.”
The H1 virus, with the L397 replacement, is the one predominantly circulating in heavily vaccinated China that has over 100,000 cases of measles per year.
Mutant strains are a real life concern to many measles scientists, because they know that wild viruses evade measles vaccine-induced antibody. They know that a high percentage of cases are vaccinated with two or three measles-containing vaccines and they know that the sera of those vaccinated do not always neutralize the wild virus. This gives the virus an advantage to mutate in the vaccinated person because it is not rapidly neutralized in the vaccinated person, in the same way that antibiotics cause bacterial mutation, when target bacteria are not effectively killed.
We know the same thing is occurring to a much greater degree with the mumps vaccine today, as evidenced by two former Merck virologists, who are suing under the False Claims Act, saying that Merck lied and consistently and illegally inflated the stated potency of its mumps vaccine. Part of how Merck allegedly committed this fraud was to test the vaccine against the weakened vaccine strain, because vaccine stimulated antibodies no longer neutralize the wild virus sufficiently to pass Merck’s tests. This is giving mumps virus an adaptive advantage within the infected vaccinated population.
There was a very interesting study[48] done in 2000. Dr Klingele et al. looked at the resistance of different strains of measles virus (both wild and vaccine strains), to the sera of two different groups: naturally immune mothers from Nigeria and 12 year old vaccinated children from Luxembourg. They wanted to see the ability of the blood of the two groups to neutralize measles virus in vitro.
They showed an inferior ability (“considerable difference”) of the vaccinated children’s sera to neutralize wild type virus vs. vaccine virus, compared to the naturally immune mothers.
“Although both cohorts were matched for their hemagglutination inhibition and standard neutralization titers, 12 of the 22 late convalescent sera, and only 6 of 24 vaccinees neutralized all viruses. Similarly, only 2 of 20 viruses were not neutralized by at least 75% of late convalescent sera, in comparison to 10 of 20 viruses that resisted neutralization by at least 75% of the vaccinees.”
The scientists concluded that there is a qualitative difference rather than a quantitative one between the vaccinated and naturally immune groups.
“Whether differences in neutralization capacity can be attributed to antigenic diversity of wild-type viruses and the introduction of world-wide immunization with vaccines of limited diversity as suggested before requires further investigation.”
Sanders[49] and others, however say, it is nearly impossible for vaccines to not cover all measles virus because of the characteristic and stability of the H protein.
But Schrag[50] also documented a different point mutation on an H gene that prevented monoclonal antibody from binding to the H protein. On the heels of reassurance that point mutations in measles viruses will unlikely ever become a real-life problem, Schrag ends with:
“In the context of measles virus elimination efforts, evidence for a high mutation rate suggests that the possibility of strains that may escape neutralization by vaccine must be considered.”
It is written that the H protein would be the most likely source of trouble if the right part of it were to mutate, and that while mutations do happen, they seem to be clinically insignificant, at least in the ways they have been tested. But is the H protein antigenic stability all that is needed to prevent vaccine escape mutations?
Kweder[51]showed that mutations not JUST in H but in H, F, or M proteins could facilitate resistance of measles virus to neutralizing human anti-MV sera. They concluded that immune resistance is due to particular mutations that can occur in any of these three proteins that affect at a distance, rather than directly, the native conformation of the MV-H globular head and hence its epitopes. Kweder said that the H, F and M proteins act in concert in an infected cell and thus their interactions being thwarted could potentially allow mutations other than in the MV-H globular head to have an effect on MV-H epitopes. And those mutants in any of the three genes for M, H and F proteins could allow escape from neutralization by anti-MV sera.
How did they get this information? They took a strain of wild measles G954 or a strain of vaccine virus and put them under selective pressure in vitro using sera from healthy vaccinated persons. Mutations were produced, and many of them were SSPE mutants.
Then . . . like all the other papers, they conclude by telling us that while these things all happen in the petri dish, they don’t happen in bodies because when they put the mutant virus against human serum from MV vaccinated donors, all was well. But alas, they admit:
“If vaccinated individuals nominally protected by anti-MV antibody are susceptible to wt MV strains, this raises concerns not only for neurological complications of MV but also for its global eradication. That wild–type MV can also accept mutations that do not compromise receptor recognition but allow immune escape underlines the importance of maintaining the monitoring of new emerging strains of the virus.”
Other literature is emerging that questions the stability of the measles virus in highly vaccinated populations where significant immune pressure can be placed upon circulating viruses, by virtue of the virus infecting more of the vaccinated asymptomatically. A paper from 2011 by Shi[52] looked to see the genetic variation in wild type measles viruses and they found it is becoming significant enough to be thinking of the “new golden era of vaccines” and to ramp up the current vaccines and bring in some new ones in order to get around the growing problem of antigenic drift among highly vaccinated populations.
China has a vaccination rate of infants between 98.5%-99% depending on where you look. Shi says 98.5% and even as the vaccination rate has climbed, the measles case rate has had resurgence. China has had a two-dose schedule since 1990.
Shi found that infants who were recently vaccinated had a four fold lower ability to neutralize wild type viruses compared to vaccine viruses, and he voiced concern that the current vaccines are not effective against circulating wild-type strains. In addition he documented the genetic drift as significant in the H and N genes between vaccine and wild viruses, and suggested that the drift is one reason for the increase in numbers of measles cases reported in China recently.
Worse yet, is that infants had the highest occurrence of measles cases followed by those aged 1-2 years. Why is this worse? Because those infants were once protected by mothers who had natural immunity and now they are not. And now those 1-2 year olds are not even solidly protected by vaccines that contain virus that is so different from the wild types circulating, that those infants are developing measles at the very age where neurologic problems are most frequent. Ironically, this is the reason we are told we need to vaccinate – to protect those young people!
The death rate had already declined significantly in the developed world before measles vaccines, when lifelong “herd immunity” was well established by the age of 15. Then the public was told they need to take vaccines in order to protect the young from neurologic diseases. But it turns out that even in highly vaccine-compliant populations, the vaccinated people themselves are able to put pressure on the wild type viruses in such a way that the vaccines no longer do the job.
Shi came right out and said of the 14 out of 16 cases that were fully vaccinated who were tested:
“These data suggest that the 16 patients from whom the 16 measles strains were isolated were susceptible to wild-type measles virus infection, perhaps resulting from the mutations of the wild-type measles virus.”
Circulating wild strains were only 16-36% related to the approved vaccine strains, which included the Edmonston strain. This paper is a game changer in terms of the pro-vaccine insisting that the vaccine covers all wild strains. Just as all vaccines and antibiotics fail over time with mutation pressure, so is the measles vaccine doing the same with circulating measles viruses.
“The genetic alterations in genotype H1 MV isolates and the resulting antigenic changes may have contributed to an increase in the incidence of measles cases observed during this outbreak in a highly vaccinated population. . . mounting evidence indicates that genetic variability occurs in wild-type strains, and existing vaccines may not be able to effectively protect populations from measles variants. . . antigenic variation may lead to the escape from immune protection elicited by existing vaccines.”[53]
In order to determine this, other countries will have to start testing the way that China has done.
Without doing that, nobody can be sure that mutant viruses that are resisting vaccinated persons’ sera are not circulating. Does anyone know if wild viruses infect partially immune vaccinated people, mutate inside them, and then are released into the community, only to continue the cycle? The only way to know would be to test every person with a measles-like disease to analyze the genotype changes on the important proteins. Is this being done? No. What about all the secondary vaccine failures or the ‘subclinical cases’ in the vaccinated?
Measles virus can circulate in vaccinated seropositive populations and naturally immune persons, once the protective level of immunity drops. Studies show that they can either manifest as secondary vaccine failures and be clinical cases, or they can just be secondary immune responders and asymptomatic. Peter Aaby[54] acknowledged that in the early days of his work in Africa, that measles disease was common in the vaccinated, and the fact that the measles was milder than normal, and “worked as an encouragement to immunisation”. So even then, they knew that the vaccine did not protect against all circulating wild strains when vaccination starts. He said,
“ ‘Mild measles’ may be a better demonstration of the value of immunization, than invisible notions like ‘permanent protection’ or ‘lifelong immunity’…”
These mildly infected, or asymptomatic people are likely shedding virus without knowing it, and are likely candidates for transmission.[55] Naturally immune persons in low circulation areas, probably always had had the ability to pass on viruses, but back before vaccines, most babies were protected by naturally immune mothers, and breastfeeding added another level of protection beyond the placental transfer of immunity from the mother.
Today, not only can naturally immune persons be asymptomatic vectors —but so can the vaccinated. Because vaccine-immunity is weaker and shorter lived, vaccinated persons are more likely vectors. Several studies show that these partially immune people can be protected from disease but not from infection.[56] In the era of vaccination we have an added problem and that is that antibody titers are lower and more likely to wane than after wild-type infection.[57] According to Damien, susceptibility to secondary subclinical immune response is 5-8 times higher after vaccination than after natural infection.[58] So, if measles continues to circulate among vaccinated people, we have created a new environment for wild measles virus—one where vaccine escape mutation is more probable.
It is well known with any infection that if the host is immune-compromised or otherwise unable to clear the virus rapidly, the microbe has an adaptive advantage and can live longer, replicating and mutating in attempt to evade the immune system. The vaccinated give the microbe the advantage in mutation capacity. This has already been well established in the case of Pertussis bacteria, where the vaccinated have cultivated a new mutant strain, because their immunity in the lung is weaker than naturally immune. Over time, a different picture of population dynamics and infectious microbes emerges, and it is often not a picture that the original designers of the vaccine programs thought of. Because of concerns that public health can be jeopardized if too many people stop vaccinating, “any possible doubts, whether or not well founded, about the safety of the vaccine cannot be allowed to exist”.[59] This historical statement is also true when anyone today expresses doubts about vaccine efficacy, not just safety.
In the past, when wild virus infected those between 2-15 years of age, natural immunity was developed. As those people aged, they were exposed to wild virus and sometimes could be sub clinically infected. But nowhere to the degree that the vaccinated have proved to be doing today:
“In a fully vaccinated population asymptomatic secondary immune response was found to be as high as 66%”[60]
Dr. Diana Griffin has stated of the live attenuated vaccines for measles that inoculation of this virus into primates produced no clinical symptoms, no detectable viremia and no spread to the respiratory tract.[61] Like the pertussis vaccines, the measles vaccine does not give strong local immunity in the respiratory tract, and thus it can be deduced that the vaccinated will not have the same level of resistance upon re-exposure and that is exactly what has been noted in numerous pertussis studies. But this has not been investigated with regard to measles.
Why is this important? For the same reason that antibiotics create mutant bacteria, and do so more effectively in those who are treated longer, allowing the surviving bacteria sufficient time to outwit the antibiotic and change its characteristic. With antibiotics and antibacterial vaccines, this is a reality that happened relatively fast.
With viral vaccines, due to the character of the microbe and immune interaction, the time frame for occurrence has been much longer, but it has begun.
Claim #6: Antibodies are useless
Next, Dr Humphries launches into a discussion on the questionable role that antibodies play in the body’s immune response, implying that vaccines (which stimulate antibody production) are in fact useless:
We’ve addressed this below within claim 7. There is no mention or implication that antibodies are “useless.” The quotes “Isabella B” used from Dissolving Illusions demonstrate clearly how “Isabella B” misrepresents our discussions.
Scientists were surprised when they learned that individuals with a deficit in antibody production recovered from measles just as well as normal antibody producers. […] Therefore the antibody part of immunity is not at all necessary for the natural recovery from measles (p 364).
And:
People without antibodies can be completely protected from clinical illness by cellular immunity. Therefore antibody is a mere surrogate that has questionable significance (p 389).
While it is true that other immune mechanisms kick into place when an individual suffers from compromised antibody production, this does not mean that antibodies are useless in otherwise healthy individuals. The study she cites in fact concludes:
Although our findings support a limited role for humoral immunity in the control of replicating virus in measles virus-naive hosts, antibody can certainly mediate protection against measles virus infection.
Furthermore, since the measles vaccine contains a live (albeit weakened) virus, it elicits a full adaptive immune response, including the complex interactions between antibody-mediated (humoral) and cell-mediated (cellular) immunity. Simply because physicians typically use antibody count as a measure of immunity does not mean that vaccine responses are limited to antibody production only. The role of cell-mediated immunity in immune responses to the measles vaccine has been extensively measured in studies like this one. See section #9 below for a more detailed discussion on this matter.
Claim #7: Antibodies are harmful
Next, Dr Humphries goes on to say that antibodies are not only useless, but in fact harmful:
It is a little-known fact that any antibody, even a vaccine-induced one, can render a person more vulnerable to disease (p 366).
Never did we imply or state that vaccines that stimulate antibody production are useless. The section emphasizes that testing for immunity and vaccine response is not a rational means to evaluate immunity since immunity to measles occurs in the absence of ability to manufacture antibody. Cell mediated immunity is all that is needed to recover from measles. Our book says:
“Scientists were surprised when they learned that individuals with a deficit in antibody production recovered from measles just as well as normal antibody producers. […] Therefore the antibody part of immunity is not at all necessary for the natural recovery from measles” (p 364).
And:
“People without antibodies can be completely protected from clinical illness by cellular immunity. Therefore antibody is a mere surrogate that has questionable significance.” (p 389)
Again the description of antibodies as useless is another figment in “Isabella B’s” imagination.
The focus of vaccination science is primarily to induce a measurable antibody response, despite the fact that other more specific cell-specific measuring technology exists.
Dissolving Illusions discusses the fact that measles patients without the ability to make antibody, fare just as well with measles as people with a ‘normal’ antibody response.
“One of the most disconcerting discoveries in clinical medicine was the finding that children with congenital agamma-globulinaemia, who could make no antibody and had only insignificant traces of immunoglobulin in circulation, contracted measles in normal fashion, showed the usual sequence of symptoms and signs, and were subsequently immune. No measles antibody was detectable in their serum [the water part of blood minus clotting factors and cells].”[62]
Why was that the case? The point that parents need to remember is that everyone, in order to recover from any infection they have never met before, uses the primary immune defense which is the innate immunity composed of a cellular immune system and some preformed non-specific antibody.
The cell-mediated immune system is also a key to rapidly overpowering and removing the measles virus from the body, and quick recovery from measles. The fact is, that measles antibody response is not necessary to survive measles infection, or to develop memory immunity. Agammaglobulinemics have long lasting CMI immunity after recovering from the infection.
If the development of IgG antibody, BEFORE infection, was necessary for recovery, or to survive, no-one would ever recover from anything for which they didn’t have prior immunity or cross protective memory immunity, also called heterologous immunity.
We also quoted Dr. Casadevall’s article which states:
“A paradoxical observation involving AMI [antibody-mediated immunity] is that specific IgG is often made after the host has recovered. In fact, a rise in serum IgG titer is a time-honored method for diagnosing many infectious diseases. This observation begs the question of why IgG is made after recovery from most infectious diseases. Invoking a need to prevent recurrences is a somewhat unsatisfactory answer if the initial innate and cellular response was adequate to clear the first bout of disease.[63]”
Preformed measles IgG antibody, while part of the natural immune response is the LAST thing to happen during recovery. These other aspects of the immune system are not commonly mentioned when vaccination is discussed, because the focus is on a myth that vaccines provide the only reliable and safe method to “become immune”, and because IgG antibody is held up to parents, as the successful measure of immunity in vaccinology.
It is just as well that we are not dependent on antibodies for survival from infection or injury in general, otherwise a lot of nephrology patients would be in serious trouble because of the very high numbers who never make high antibodies after vaccines are given to them. It’s also nice for a nephrologist to be able to reassure patients that their lack of ability to make antibodies isn’t going to be the thing that stops them fighting and surviving acute illness.
This is basic immunology 101, which any parent with common sense can understand.
Nowhere is there an insinuation that antibodies are useless. The implication that Dr. Humphries is saying “antibodies are useless” is another product of “Isabella B’s” fictitiously orientated intellect.
And:
Some antibodies increase the ability of viruses to infect their target cells. This phenomenon is called antibody dependent enhancement (ADE) of infection (p 367).
This may sound alarming but she fails to mention that the “ADE phenomenon” described above is incredibly rare and has only been observed in relation to the particular characteristics of the dengue fever virus and HIV virus. It is not a phenomenon that relates to the viruses we currently vaccinate against — measles, mumps, rubella, chickenpox, rotavirus and influenza.
We could have written so much more about the fascinating topic of ADE, but to keep the book from being an encyclopedia we didn’t.
The purpose of the discussion of ADE was to detail the extraordinary complexity of an immune response and how things may not always turn out as planned.
“Isabella B” apparently completely missed out on the discussion of a well-known and well described phenomenon called “antibody dependent enhancement” as meticulously described in Dissolving Illusions’ measles chapter. Moreover she did not understand the following from page 367 of Dissolving Illusions where ADE was discussed.
“There is no controversy over the fact that the inactivated measles vaccines led to an abnormal immune response and, later, a form of original antigenic sin. Several mechanisms have been proposed over the years.”
Note the description “inactivated measles vaccines” as in the killed measles vaccines that were discussed in detail in the preceding pages. In no way was there an implication that today’s live attenuated measles vaccines cause ADE. Such a conclusion is again, a fantasy of “Isabella B” or a result of her inability to identify adjectives and read clear scientific and historical descriptions.
The fact is— the official documentation of the true impact of ADE was quite poor.
The killed vaccines were used until 1967, and according to Dr Anthony Morris, former FDA vaccine safety scientist, “Literally millions of children were vaccinated with that [inactivated] vaccine.” The official record is that “only” 600,000 to 900,000 children[64] received the killed vaccine. Dr. Cherry noted that many diagnoses of atypical measles were missed by doctors because they didn’t know what it was they were seeing. While many say the problem was only from 1963 to 1967, they are incorrect: Dr. Cherry said in 1980:
“In the years to come, still more cases undoubtedly will occur, and in many the etiology will go unrecognized.”[65]
Dissolving Illusions’ authors in no way meant or implied that antibodies never do any valuable immunologic work. They do. But in the case of the early measles vaccine, that was highly lauded by the vaccine faithful as helpful, the antibodies that the killed vaccine produced, turned out to put the vaccinated at a great disadvantage. This is a little known fact amongst doctors and parents despite it being plastered throughout the measles medical literature.
Dissolving Illusions is a book on the history of disease and vaccination. ADE is an important piece of measles vaccine history.
CLAIM #8: THE MEASLES VACCINE WAS NOT RESPONSIBLE FOR THE DECLINE IN THE DISEASE
The data clearly shows that the introduction of the measles vaccine brought with it a tremendous (98%) drop in measles cases in the United States over the course of a few years.
This data does not sit well with Dr Humphries. She argues that, since vaccination coverage was only 50–60% in 1968, the year the live measles vaccine was introduced, the measles vaccine could not have had any effect.
This is what Dissolving Illusions says:
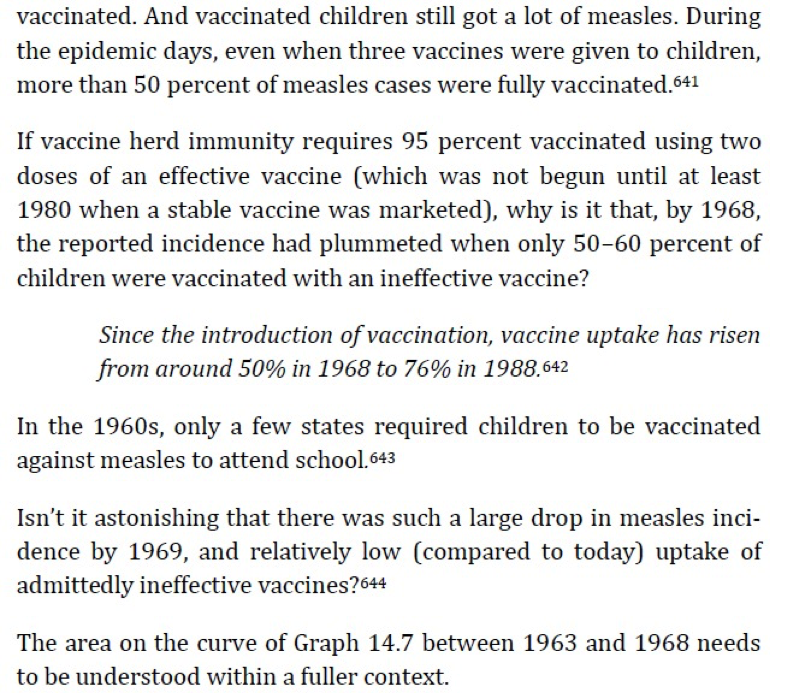
No epidemiologist worth their degree would argue that the decline in cases was solely due to the vaccines used in the first few years.
But “Isabella B” says that even though measles deaths were extremely rare, measles incidence did have a “massive landslide” after 1963—so the vaccine must be solely responsible. The issue is more complicated than she understands.
First, the data portrayed in the graph that Isabella used in her blog (seen again below) shows that there was a decline in reported measles cases in the USA before the use of any vaccine. We discussed this in more detail above in “claim 1”.
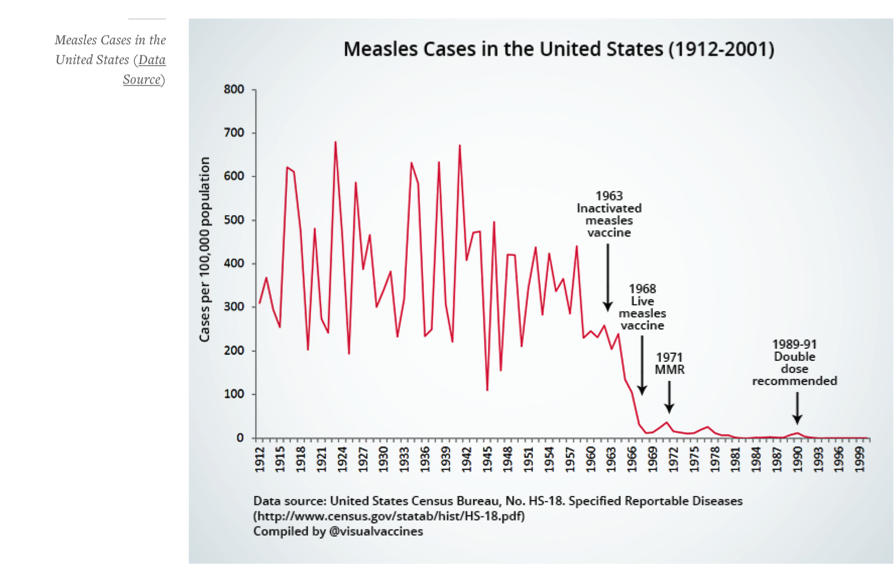
Second, after 1963, you could be infected and clinically symptomatic with a vaccine virus (or a still circulating wild virus) and you would not be counted as having measles because you were vaccinated, just as happens today. There is a case from California where a child was counted as a measles case[66] until she got home to Alaska, whereupon, because of enhanced surveillance, she was diagnosed as having vaccine-strain measles and thus retracted from the measles count. The same occurred in a Canadian baby who was struck from the record after the diagnosis of vaccine-strain clinical measles.[67]
“Isabella B” says:
While it is true that an 80–90% immunization level is needed to maintain the phenomenon of “herd immunity”, it is obvious that even a moderate vaccination uptake would have made a significant dent in the disease’s incidence and transmission rates.
How is it obvious? We have the highest ever pertussis vaccine uptake and supposed herd immunity, and yet the circulating whooping cough infection rates are higher now, than the prevaccine era.
“Isabella B” has fallen behind the news in the fantasy world of assumed community protection vaccination rates for the illusory “measles vaccine induced herd immunity”. The recent level needed to vaccinate is 99%!
“Given the highly contagious nature of measles, vaccination rates of 96% to 99% are necessary to preserve herd immunity and prevent future outbreaks.”[68]
Dr Humphries then offers these alternative theories for the dramatic decline in measles notifications in the 1960s:
a)Doctors changed their diagnostic criteria. In other words, Dr Humphries complains that “there are at least 10 other infections that clinically resemble measles”. Her assertions implies that 1) physicians in the 1960s who were intimately familiar with measles suddenly became incompetent at diagnosing it from one year to the next, and / or 2) all healthcare workers were wrapped up in a global conspiracy to “hide” disease notifications and give the vaccine a semblance of effectiveness where there was none. This theory requires the suspension of disbelief. Since measles is highly contagious, it is unfathomable that all physicians would be careless enough to dismiss genuine measles as “some other rash” merely on the basis of population-wide vaccination rates.
If readers will refer to pages 370 – 373, where the explanation is detailed with references, they will see for themselves, that the above “global conspiracy” allegations are another fictitious figment from the conspiracy addicted imagination of “Isabella B”.
In the post vaccine era, if a vaccinated person contracted measles, they are not counted as a measles case, even if they had a serious case of measles. There was no genotyping of the infected virus, so the case had to be linked to a proven measles case. It is well known and accepted, that the measles vaccine gives a subclinical case of live measles, which results in interruption of wild measles transmission. That’s why we have low levels of wild measles today.
Today, all clinical cases of measles in vaccinated people are genotyped, and if the virus in the infected person is a vaccine virus, that case is struck from the record.
b) Use of gamma globulin (passive antibody) as a treatment for measles to eliminate rashes. This, however, is no longer in use since 1968.
This comment above is totally false. The case of a vaccinated child who tested positive for vaccine-strain measles infection in Canada that Murti wrote up in 2013[69] provides evidence that “Isabella B” is wrong. All 45 susceptible contacts exposed to that child received a vaccine, immune globulin or both. When doctors or health authorities panic, the immune globulin is used today. CDC[70] and other various health providers[71] [72] in the USA have their own guidelines for the use of immunoglobulin for measles.
However, the point made in the measles chapter was that between 1963 – 1968 doctors were supplied with live measles vaccine that caused high numbers of febrile and symptomatic cases. Doctors were so afraid of this vaccine that they usually gave immune globulin simultaneously. Again this is well documented, and the practice did not stop until a well-attenuated vaccine was available years later in 1968.
Photo above courtesy of the College of Physicians of Philadelphia site, history of vaccines.[73]
The whole point in mentioning immune globulin in Dissolving Illusions, is that its use from 1963 to 1968 helped the vaccinated cases appear less sick, even though they had clinical measles, and without injected gamma globulin, would have been quite ill. Thus these modified measles cases were never counted as measles cases, and helped to create the “landslide” decline that “Isabella B” notes in case reports, post-vaccine.
The fact is that true herd immunity that lasts a life time, created by wild measles, was replaced by an infectious virulent injection of laboratory cultured measles virus and the resulting infections were no longer notified as measles.
“Isabella B” says Dissolving Illusions implies the following:
The incidence was already on a decline. Like smallpox, she claims, the disease was “slowly burning out”.
No, on page 374 the question was asked “was the disease slowly burning out?” Measles was described as a mild disease in 1959, in the BMJ. The question is, was it becoming less virulent, so much so that a case might not be recognized?
Our point was, that as the 1959 BMJ article showed, the disease was less problematic on the whole, when it was naturally coursing through society in developed countries, and the focus could have been on developing proper treatment and immune system support rather than a lifetime of vaccines, which is what the public has ended up with today. How often has anyone read or heard the CDC mentioning any other means to support or deal with any disease other than hand washing and vaccines?
I don’t know about you, but this curve definitely does not look like a disease slowing burning out. It looks like a massive landslide:
Once again this “landslide” was not in fact due to a killed measles vaccine and a virulent live vaccine plus immune globulin, which were the only vaccines available until 1968. We describe this above. In the beginning years, this landslide was mostly just reporting artifact.
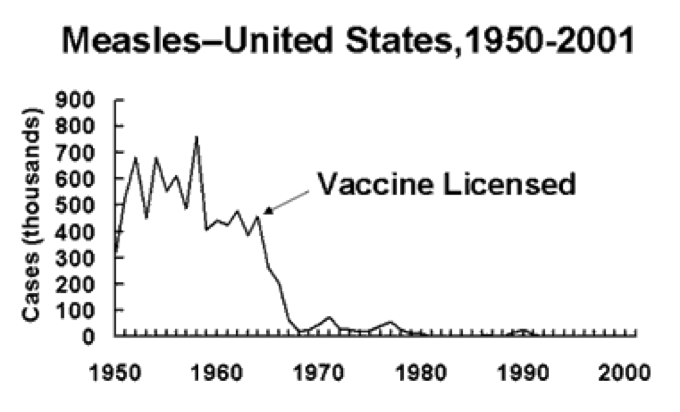
We need to repeat this important point again. “Isabella B” fails to mention the most important thing: that measles mortality had declined by over 98% in the United States by the time the first vaccine was introduced. Our book is criticized because we talk about death rates more than incidence. But, decline in death rate was, and is, one of the best, and most highly significant markers of overall health improvement. That is why all countries measured their progress by death decline, and increased lifespan.
That is why when doctors get angry because you won’t accept a vaccine, drug, or test, they often say, “But your baby might die!” In 1994 when the UK parents were coerced into a mass vaccination campaign, the threat of death, not encephalopathy or blindness, was used as the main tool to increase compliance. The Bulletin of Medical Ethics August 1995[74] detailed the whole sordid event.
Again, isn’t it fascinating how the “landslide” reduction in the very measure used to scare parents into vaccinating (death), is suddenly now considered insignificant by “Isabella B”? Isn’t it interesting that interventions that so markedly reduced the death rate (hygiene and nutrition) get no credit, unless a pharmaceutical corporation developed it?
| Looking at data from pre-vaccine England, the mortality rate had declined by nearly 100%. The medical literature of the time indicates that measles by the 1950s was generally considered a mild disease. By 1962[75] in the UK, there were 184,895 measles cases and 39 deaths, which = 1 death per 4,740 cases. Yet now, the CDC says that “For every 1,000 children who get measles, one or two will die from it.”? If so, what has gone wrong here? |
The USA data for 1962 measles according to CDC[77] is as follows:
“In the decade prior to the licensure of live measles vaccine in 1963, an average of 549,000 measles cases and 495 measles deaths were reported annually. However, almost every American was affected by measles during their lifetime; it is estimated that 3-4 million measles cases occurred each year.”
495 deaths in 4 million = 1 death per 8,080 cases of measles. Again, that’s a far cry from CDC’s current information page stating 2 deaths per 1000 cases.
CLAIM #9: RASHLESS MEASLES LEADS TO DEGENERATIVE DISEASE
Next, Dr Humphries speculates that measles antibodies (derived from vaccines) interfere with a cell-mediated immune responses to the wild virus, leading to chronic measles infection and eventually immune related disorders later on in life:
Acute natural infection and presumably even vaccination during a time when measles-specific antibody is present may induce a longterm suppressive effect on measles immune response. The presence of such antibodies at the time of infection interferes with the cellular immunological response to measles virus, especially with the development of specific cell-mediated immunity […] Intracellular measles virus may then survive the acute infection and later cause diseases which develop in adulthood.(p 383).
Her proof rests on a 1985 Lancer paper entitled “Measles Virus Infection without Rash in Childhood is Related to Disease in Adult Life”. This is a frequently misquoted paper because it is access restricted and has an obscure sounding abstract. After paying the $35.00 to access the full report, I realized that it did not study the effects of measles vaccination at all. It was a historical study done on individuals born in Copenhagen and Gentofte in the pre-vaccination era — specifically 1941 and 1947 onwards. It found that individuals who had contracted the wild form of measles (measured via antibody levels later on in life), without manifesting a rash (roughly 9% of the population), had a higher incidence of degenerative diseases later on in life.
In Dissolving Illusions we discussed a Lancet paper from 1985 by Rønne titled “Measles Virus Infection Without Rash in Childhood is Related to Disease in Adult Life”.[78] It is an interesting read with important implications.
In order to throw off the virus, a brisk cell-mediated immune response is necessary. That immune response is usually visible in the skin in immune competent hosts. The rash is the immune system taking out infected cells. The extreme opposite is the AIDS patient who gets no rash and the diagnosis is not made until autopsy.
Dr Rønne reported cancers and autoimmune diseases in persons who had rashless cases. Specifically, he noted a highly significant association between a negative history of known measles with evidence of prior rashless infection (detected by antibody before and after later re-exposure) and four disease categories: immunoreactive diseases, sebaceous skin diseases, degenerative diseases of bone and cartilage, and tumors.
The study speculates that a reason for the absence of rash may have been treatment of measles with immune serum globulin (which is essentially an injection of passive measles antibodies). The author hypothesizes that an injection of passive antibodies at the time of measles infection may interfere with the body’s full immune response to the virus, leading to latent health problems.
In the end, the study recommends aborting immune serum globulin as a form of measles treatment (which is no longer in use today) and using well-timed measles vaccination to reduce the incidence of degenerative disease:
Dr Humphries completely misrepresents the study. She concludes somewhat simplistically that an “absence of rash” after measles vaccination signifies an “absence of cellular immune responses” to the virus which in turn leads to degenerative disease later on in life.
Dr Rønne said this:
“The association between a negative history of measles, early exposure (possibly injection of ISG [immune serum globulin] after suspected exposure), specific measles antibodies in adulthood, and nonmeasles associated diseases, suggests that the presence of measles virus specific antibodies at the time of infection interferes with the common immunological response to measles virus, especially with the development of specific cell-mediated immunity (and/or other cytotoxic reactions). Intracellular measles virus may then survive the acute infection, and cause diseases which develop in adulthood.”
There it is, in Dr Rønne’s own words. How was the study misrepresented?
Other immunologists since then have agreed that preformed specific antibody actually limits cell-mediated immune responses. The reader must understand that antibody alone without T cell immunity does not happen with normal measles. Normally there would be an infection, a cell mediated immune response, followed by IgG accumulation. This is not to say that preformed antibody does not have immediate protective influence against measles. It does. This is WHY it is and was used in the past after exposure or with poorly attenuated vaccines.
An out of order immune response has implications for early vaccination of infants who still have maternally transferred specific antibodies, which is done in the USA in special circumstances, and in the developing world routinely. It also has implications in terms of the use of immune serum globulin upon exposure, which is still used today, AND was used alongside the live measles vaccines from 1963 to 1968.
Uhlmann[79], Walker[80] and others[81] have shown residual intracellular measles retention in vaccinated populations with autism and enterocolitis. This phenomenon is obviously the result of a muted, inadequate cellular immune system response to the vaccine virus. Why does it happen? And more important, why is the study of this subject not well funded and aggressively investigated?
However, contrary to the 1980s, we do not need to speculate about whether the measles vaccine stimulates cellular immunity or not — we can measure it. The measles vaccine stimulates a full adaptive immune response, involving both antibody mediated and cell-mediated immunity:Even decades after measles immunization, both the CD4+ and CD8+ T-cell pools contain high levels of measles virus-specific memory T cells. This indicates that measles vaccination induces a long-lived T-cell memory response. (Source)
Dr. Gregory Poland has written extensively[82] about how in terms of cell-mediated and humoral immunity, we are genetically and epigenetically different to each other, and these differences mean that the measles vaccine as it is today, cannot eradicate measles, because of the large number of primary and secondary vaccine failures. He thinks we need a new vaccine. And he loves vaccines.
Poland’s laboratory (Dhiman[83]) looked at the precise immune responses of 346 individuals (12- 18 yrs of age) who had two doses of MMR-II vaccine.
They detected NO immune reaction at all in 1.2% of subjects; a humorally biased response ‘characterized by the presence of antibodies and IL-4 and undetectable IFN-γ and lymphoproliferative response’ in 7.4%; and a Th1 biased response in 1.2%.
All of those subjects reacted outside of what is expected, with 8.6% not generating a full adaptive memory T cell response like “Isabella B” says they should, and 1.2% with no immune response at all. That makes nearly one out of ten children whose immune systems are inappropriately skewed. One out of ten children is very significant
We never deny that cell mediated immunity occurs after vaccination. We discuss it in the book, and are aware of just how complex the immune response is. We are also aware of the abundant medical literature reporting that there are both primary and secondary vaccine failures (8.9% of twice vaccinated healthy children[84] lacking protective levels of circulating antibodies) because the vaccine does not come close to the specific strong cellular immune response of an inhaled natural virus. This is of course why Dr Poland[85] is at the forefront of a move calling for a ‘new golden era of vaccinology’ where new vaccines should be developed to overcome ‘aberrant immune responses’. Dr Poland states clearly that measles cannot be eradicated with the current vaccine.
| There is a study by Pabst in 1997 (Pabst 1997 PMID: 9475303) that is very relevant to this conversation because his blood testing showed that babies who were formula fed and MMR vaccinated had an entirely different response to vaccination than breast fed babies. They also had markedly different immunologic phenotypes from each other before vaccination. His tests revealed that formula fed vaccinated babies had an erratic immune system characterized by high antibody levels and chronically activated T cells of low efficiency. Breast fed babies had a targeted and brisk T cell response to the MMR vaccine, and low antibodies.
One of his concluding remarks is: “conditions favouring antibody responses to viral infections may be accompanied by inhibitory cells that downregulate cell-mediated immunity.” Pabst (Pabst 1990 PMID: 1973970) also stated: “Breastfeeding enhances the active immune response in the first year of life and therefore the feeding method must be taken into account in the evaluation of vaccine studies in infants.” And that is some thing that “Isabella B” and parents need to get their heads around, because under certain conditions, injection-induced antibodies can indeed limit the cell-mediated immune response to measles. |
While “Isabella B” tries to portray us as irrelevant liars with no understanding of the immune system or the measles virus’ interaction with it, we can assure you we have done our homework. As has Dr. White[86] who says the following:
“Immunological profiling of vaccines in human infants has traditionally relied principally on measurement of humoral immune responses, and despite a consensus that vaccine side effects are more likely to involve aberrant cellular immune responses (CMI) there are no statutory requirements for provision of CMI data as part of either safety or immunogenicity testing.”
Dr. White also mentions that the immune response is so complicated as to activate hundreds to thousands of genes.
“Isabella B” is working hard to make the case that we used the study to say that vaccines only make antibody and that that makes vaccinated people like the subjects of Rønne’s study. Here is what we concluded:
“Those children who received ISG (immune serum globulin), after 1941 and through the 1960s and 1970s and, in some cases, even today as part of measles prevention, were/are most at risk.”
AND . . . “It is well known that infants do not respond in the desired fashion to a vaccine given in the early months of life, and if they are vaccinated too early (before 15 months of age) they can become nonresponders even after revaccination.”
Then we closed with a series of questions that are largely unanswered. Poland and associates are well aware of the limitations of scientific measures. Today’s vaccinologists are well aware of the diversity of human epigenetics, and that the consequences of vaccination are determined by those epigenetic, genetic and environmental differences, AND … the order in which vaccines are given. Rønne’s study was interesting, and still has relevance.
Can anyone be assured that autoimmune and cancer epidemics we face in the developed world have nothing to do with vaccines? Of course not. Rønne was simply ONE researcher who looked at a specific situation and found something which is pertinent to the discussion:
“There was evidence of association between a negative history of measles, exposure in early life (possibly injection of immune serum globulin after exposure), and development of immunoreactive diseases, sebaceous skin diseases, degenerative ·diseases of bone and cartilage, and certain tumours. It is suggested that the presence of measles virus specific antibodies at the time of acute infection interferes with development of specific cytolytic reactions, and enables intracellular measles virus to survive the acute infection.”
And that is exactly the situation that applied from 1963 – 1968 in any country that used the early measles vaccines and at the same time, injected gamma globulin.
In fact, cellular immunity from the measles vaccine may even outlast antibody mediated immunity leading to long term protection:
These data suggest that cellular responses to measles virus may be better sustained than antibody titers after vaccination and revaccination in some subjects. (Source)
“Rashlessness” after measles vaccination is not related to lack of cellular immunity. It is more likely related to the decreased virulence of the virus in the measles vaccine, giving the body an easier time to fight off the pathogen.
Once again . . . we were not talking about rashlessness after routine vaccination to one-year-olds. Dhiman shows that most subjects respond with Th1 and Th2 responses. We were talking about the use of immune serum globulin in the past and present and, vaccination of babies when they still have maternally derived anti-measles antibody.
The effects of maternal antibodies on vaccine responses
There is another aspect to the 1985 Lancet paper above, and that is the possible effect of passively acquired maternal antibodies on the body’s ability to respond to the measles virus. It is interesting to note that babies receive most maternal antibodies before birth via an active transport system in the placenta. These antibodies protect the baby for several months but fade around the 6–8 month mark, depending on the amount of transplacental antibodies received. Babies are unable to absorb maternal antibodies via breast milk or colostrum into their blood stream, except in very minute amounts. Maternal antibodies in breast milk primarily protect against gastrointestinal infections and diarrheal disease, locally, in the gut. This article describes current research in the field with links to studies and sources.
Perhaps “Isabella B” doesn’t grasp just what is in human milk. Yes, maternally transferred antibodies protect the baby, but human milk also passes on numerous biologically active compounds that kill viruses, bacteria, and even mutated cells. Human milk also transfers approximately 10 trillion maternally derived living cells per day that includes activated T and B cells. There is no debate whether or not breastfeeding is protective and continues that protection that started with passive antibody transfer.
To prevent interference from latent transplacental antibodies, the measles vaccine is only given from 9 months onward. Passive antibodies decline before that age so that babies can form a successful immune response to the virus. Any hypothetical risk factors outlined in the 1985 study above are thus nullified.
Those risk factors are certainly NOT nullified. There have been trials of giving measles vaccine at 4 months of age. When the high titer vaccine was used in West Africa mortality doubled.
AND The CDC recommends under some conditions that infants 6 months old get MMR vaccines. “People 6 months of age and older who will be traveling internationally should be protected against measles.”
http://www.cdc.gov/measles/vaccination.html
AND as described below, the ACIP does recommend vaccines to 6 month old infants, and immune globulin to ALL infants younger than 12 months after suspected exposure, which makes Rønne still relevant, and “Isabella B” incorrect again.
“In the 2013 revision of its MMR vaccine recommendations ACIP expanded the use of post-exposure IG prophylaxis for measles. Intramuscular IG (IGIM) should be administered to all infants younger than 12 months who have been exposed to measles. The dose of IGIM is 0.5 mL/kg of body weight; the maximum dose is 15 mL. Alternatively, MMR vaccine can be given instead of IGIM to infants age 6 through 11 months, if it can be given within 72 hours of exposure.” http://www.immunize.org/askexperts/experts_mmr.asp
Rather than leading to “deranged immune systems”, as Dr Humphries claims, present day studies repeatedly hint at beneficial immuno-stimulating properties of the live measles vaccine above and beyond protection against measles infections:
The measles vaccine activates the immune system in a non-specific way providing protection against other infections.(Source)
Finally, “Isabella B” is correct. Yes there appears to be an immune stimulating property to some live vaccines, as well as measles infections. This is not under dispute.
Other studies also report the fact that DPT vaccines are associated with high mortality in undernourished children. Dr Aaby again:
“Ten years ago we reported in an observational study from rural areas of Guinea-Bissau that routine DTP vaccination was associated with an 84% (10–210%) increased mortality.”[87]
Vaccine enthusiasts are quick to point out the reduced long-term mortality measurements in underdeveloped countries after measles vaccines, but slow to recognize that DPT vaccines increase long term mortality, so do the exact opposite to live vaccines.
What Dr Aaby later found was that the excess mortality was due to DPT being given AFTER the measles vaccine, which neutralizes the “ability” of both the measles disease and the measles vaccine to confer the normally protective measles immunostimulation. Why are doctors in the developed world unaware that African children died BECAUSE they were given a DPT vaccine AFTER measles vaccines?[88]
Are doctors NOT giving DPT after measles vaccines in the developed world? Do they even understand the potential problem with DPT vaccines? If they think that only applies to Africa, they plainly have not followed the current research in Denmark,[89] which shows that the same phenomenon applies there as well.
Another inconvenient fact is that measles infection has the same beneficial activation that the vaccine does, as documented by Dr. Aaby. There are benefits to recovery from measles disease, which Dissolving Illusions touches on, AND which was even quite evident in the poorest sections of Africa[90].
Several of Aaby’s studies show this:
“It seems clear that there are no persistent T lymphocyte immunosuppression and no excess mortality in the post measles phase.[91]”
“The net impact of natural measles might be beneficial in situations with no acute mortality[92]”
In countries with low measles mortality (which would be the developed world), there is a long-term survival advantage of having measles infection. The other benefit of surviving normally mild measles, is that you don’t have to be revaccinated or suffer primary or secondary vaccine failure. Nor do you have to risk brain damage from the vaccine as Dr. VK Singh and others have argued the case thereof.
And:
Contrary to current assumptions, children who survive the acute phase of measles infection may have a survival advantage compared with unimmunized, uninfected children. Hence, both disease and immunization may be associated with non-specific beneficial effects, presumably due to some form of immunostimulation. (Source: Aaby 1995: PMID: 7502100)
Yes – exactly – as per the title of Dr. Aaby’s article, measles disease is good for something![93]
We are amused that you cited Aaby 1995, because a close read of that report, would reveal to readers how hollow your arguments are.
Aaby also said repeatedly that both vaccine and infection reduced long term non-measles all cause disease death.
Aaby also said that the reduction in mortality after measles immunization may have little to do with the specific prevention of measles, which pretty much shoots a hole in the “even if measles doesn’t kill you now it will kill you later” theory that is emerging in 2015.
Worse still, is that Aaby also noted that in West Africa there was an emerging problem of vaccine immunity waning very rapidly.
“Apart from popular resistance to vaccination in developed countries, the greatest threat to measles eradication might be waning immunity among vaccinated persons, resulting in secondary vaccine failure and low vaccine efficacy (Chen et al., 1990; Aaby et al., 1999 ). The rate of measles antibody decay is not very well described, but data from West Africa suggest that vaccine induced measles antibodies wane fast (Whittle et al., 1999a ). In highly vaccinated populations where circulation of wild measles virus has been interrupted, no boosting of the antibody level will take place, and measles antibody levels may decline rapidly (Mossong et al., 1999).
. . . In fact, we have already in the period 1995-1997 observed an increase in measles incidence among young adults in rural Senegal compared with the pre-vaccination era (Cisse et al., 1999). This is potentially problematic in areas with high fertility; many young women will get measles while pregnant or they will get measles together with their own children. These are the worst forms of measles: mortality is increased among pregnant women with measles (Atmar et al., 1992 )”[94]
How tragic, and all as a result of miscalculating the consequences of vaccination, and the fact that while the vaccine would stop circulation of wild viruses in time, that that has a downside, and as a result, community immunity would suffer.
If parents and doctors did their homework, and read the medical studies we have read, what would they think?
CLAIM #10: BREAST MILK OFFERS SUPERIOR PROTECTION AGAINST MEASLES COMPARED TO THE VACCINE
Next, after having argued extensively that antibodies are useless (claim # 6), harmful (claim # 7), and play a role in degenerative disease (claim # 9), Dr Humphries does a full 180 and posits that the antibodies received via breast milk offer superior protection against measles infection compared to the vaccine:
Here is some of what we mentioned about breast milk in the book:
“Breast milk is not just food, and its immunoprotective properties involve more than just antibodies. Colostrum contains viable T lymphocytes that impart immunity to the newborn.
A flood of immune cells ready and primed to do battle comes from maternal milk. Immunocompetent measles-convalesced mothers are known to transfer memory-activated T lymphocytes that have accumulated in the breast. The T cells in mammary glands are predominantly activated ones and far exceed the concentration in maternal blood. Those cells enter the infant’s intestine, pass through to infant lymph nodes, and are used by that infant to resist disease. This type of immunity is not from placental transference and is only present in breastfed infants, not formula-fed ones.
Breast milk contains stem cells, myoepithelial progenitors, immune cells, interferon, and cytokines. A vast array of “new” immune cells are being added to the list every year. There is ample evidence that breast milk has an immunomodulating effect via interferon and Th1 cell response to measles that formula does not have.
There are lower levels of virus-specific immunity in the serum and milk in vaccinated mothers compared to naturally immune mothers. Although the overall clinical case rate may have declined with measles vaccination, the most sensitive members of the herd are at an increased risk today—because of vaccination.
In contrast to a vaccinated mother, if a naturally immune mother’s infant is exposed to the virus during breastfeeding, the baby has access to the mother’s innate and acquired cellular and humoral immunity. Medical literature suggests that the lower risk of contracting clinical measles after being breastfed can last up to 10 years.”
We also put in all pertinent references, as with the rest of the book.
“Isabella B” fails to mention that vaccination has shifted the infection risk onto babies of vaccinated mothers, where in the past they were protected because those mothers had natural infection.
“Waning immunity may become an increasing problem as vaccine coverage increases: because more mothers will have been vaccinated and since they have not been exposed or had natural measles, they will transmit lower levels of maternal antibody. Thus their babies become susceptible to measles by 3 to 5 months of age.”[95]
However, as “Isabella B” notes we stated:
“When Silfverdale evaluated thousands of vaccinated and unvaccinated breastfed and non-breastfed children looking at the risk of measles, breastfeeding had a far larger impact on measles risk than vaccinating.”
This is “Isabella B’s” only valid criticism relating to the original edition of Dissolving Illusions.
We made a mistake in writing up the conclusion of the paper, which was amended in subsequent editions of the book.
Our book now reads:
“When Silfverdale[96] evaluated thousands of vaccinated and unvaccinated breastfed and non-breastfed children looking at the risk of measles, breastfeeding had a significant impact on lowering measles risk when compared to non-breastfeeding, independent of vaccination.”
Claim #11: Vitamins are all you need!
Lastly, Dr Humphries launches into a long-winded discussion on vitamin A as a miracle cure for measles:
It made no more sense to vaccinate against measles in 1963 than it does to put an infected child in a dark room instead of just giving vitamin A, which protects the retinas and the uninfected cells. (p 391)
It makes no sense to put a child with photophobia into a dark room, because that does not address the cause at all. In fact Dr. Humphries recently met an American woman in her 80s who was put in a dark room and went blind, later to have her eyeball removed, because she was not treated for the cause of her photophobia and eye pain, which was vitamin A deficiency.
There are several issues to consider regarding vitamin A, which makes the subject complicated.
- The difference in baseline vitamin A levels among different people, before being infected with natural measles.
- The effect of high dose vitamin A supplementation upon infection with natural virus, which was what the discussion in Dissolving Illusions was about.
- The effect of vitamin A supplementation at different times in infancy when a child is not infected, and the impact of different vaccines such as BCG, DPT and measles, which is an area that could be covered by its own book.
However, Dissolving Illusions, being a history book, outlined the history of vitamin A writings on high dose supplementation at the time of acute illness. Several quotes from peer reviewed medical journals were cited.
The point was that nutrition had a huge impact on the decline in mortality from measles. In countries where nutrition is poor, Vitamin A supplementation at the time of infection is even more important.
While vitamin A has proven clinical benefits in the treatment of measles, it is far from the wonder drug that Dr Humphries claims it to be. Unfortunately, deaths and complications still occur despite widespread protocols on vitamin A therapy.
Nowhere in the book was Vitamin A described as a “wonder drug” or as “all you need”. To suggest that it was is a gross misrepresentation of the book. If a child is starving, bottle-fed, or low in other important micronutrients, vitamin A will not suffice.
A Cochrane review of various studies in the field of vitamin A therapy for measles summaries the matter thus:
Eight studies involving 2574 participants were included in this review and we found that there was no significant reduction in mortality in children receiving vitamin A. However, vitamin A megadoses (200,000 international units (IUs) on each day for two days) lowered the number of deaths from measles in hospitalized children under the age of two years.
The authors conclude that vitamin A megadoses appear effective in reducing mortality from measles in children under two years old and have few associated adverse events. There is insufficient evidence to draw conclusions regarding effectiveness in preventing pneumonia or other complications in children.
While the Cochrane reviews are generally well-conducted and reliable sources of information, the limitations of what they can extract from meta-analyses should be understood.
“It is clear that the studies were heterogeneous in several ways. They were of different durations, in slightly different age groups, using different doses of Vitamin A in different formulations (oil or water-based), different settings (hospital or community), and different geographical areas with varying measles case-fatality rates.”
The report is on pooled data of randomized controlled studies. There is enough evidence that mortality and morbidity is significantly reduced, to direct WHO policy, which is to implement megadose vitamin A treatment to the regimen of acute infections.
Beyond that, Dr Christine Benn who is part of Dr Aaby’s team states the following:
“Far greater numbers of children (estimated 127 million) show no external signs of vitamin A deficiency, but have dangerously low stores, which lead to increased risk of infection and death, making vitamin A deficiency a major contributor to child mortality.
Vitamin A supplementation is considered among the most important tools to reduce child mortality in low-income countries. Recently a series of papers on maternal and child under nutrition were published in The Lancet. It was concluded that “Of available interventions, counseling about breastfeeding and fortification or supplementation with vitamin A and zinc have the greatest potential to reduce the burden of child morbidity and mortality.” The Copenhagen Consensus 2008 aimed to set priorities among a series of proposals to confront great global challenges. Vitamin A and zinc supplements for children were ranked the top priority.
To increase vitamin A supplementation coverage, WHO recommends integration of vitamin A supplementation with the Expanded Programme on Immunization. During the last decade the coverage of vitamin A supplementation has increased dramatically. The WHO vitamin A supplementation policy picked up steam after a number of randomised community-based trials in the late eighties and early nineties (10-18) had shown that high-dose vitamin A supplementation to children between 6 months and 5 years of age reduced overall mortality. Several meta-analyses estimated that vitamin A supplementation could decrease mortality by an impressing 23-30 %.”[97]
In Dissolving Illusions, we focused on the use of vitamin A for ACUTE measles treatment and the negative effect measles infections can have in vitamin A depleted people.
We never made any claims that vitamin A reduces pneumonia. There is no controversy about the need for vitamin A in acute measles. If “Isabella B” is attempting to argue that there is controversy, “she” is totally out of touch with the medical literature, and is in opposition with WHO policy.
Dr Humphries then claims that the measles vaccine similarly depletes vitamin A levels in children and leads to illness, stating:
The vaccine does deplete vitamin A stores. This is well documented.
“Previous studies have shown excess mortality and immune abnormalities among girls immunized with high titer measles vaccine 2 to 4 years after immunization . . . our results showed that serum vitamin A concentrations were depressed after measles vaccination, irrespective of whether it was the monovalent or combined measles vaccine.”[98]
“Serum vitamin A levels are reduced following vaccination with monovalent and combined live attenuated measles vaccines.”[99]
Measles vaccine has been associated with other unexpected adverse findings in long-term studies. In developing countries, the use of high-titre vaccine at 4–6 months of age was associated with an unexpectedly high mortality in girls by the age of 2 years from infectious childhood illness. (p 395)
However, this statement is completely untrue. The study in question actually compared the effectiveness of the high-titre versus standard-titre measles vaccine, using mortality rates as the comparative metric. It found that the standard-titre vaccine was simply more effective in reducing mortality rates, especially in girls:
The point was that higher titer vaccines DID cause a huge increase in mortality. This may be an inconvenient piece of information for “Isabella B”, but twisting it to mean that the lower titer vaccine was simply more effective is very misleading. In fact the lead author of all the studies, Dr. Peter Aaby in 2011 has this to day of the high titer vaccine:
“However, long-term follow-up of cohorts in Guinea-Bissau and Senegal found that HTMV [High-Titre Measles Vaccine] was associated with two-fold higher mortality for girls but not for boys. A meta-analysis of HTMV studies from West Africa showed an overall 33% increase in mortality between 4 and 60 months of age and an 86% increase for girls. Assuming the same effect in other settings in Africa and a 50% coverage for measles vaccine, the use of HTMV would have meant ½ million female deaths a year merely in Africa had it not been withdrawn. . . HTMV could have become a disaster if it had not been withdrawn.”[100]
A “disaster”! “Isabella B” is just plain wrong in her mental contortion to protect vaccination at all costs.
Holt et al. in 1993 said:
“the remarkable similarities in the pattern of female-specific increased delayed mortality in high-titer vaccine recipients in this study and the studies from Senegal and Guinea Bissau cannot be dismissed. In April 1992, a preliminary data set from our study and data sets from several other high-titer studies were shared with Paul Fine and Jonathan Sterne of the London School of Hygiene. Their meta analysis revealed an overall increased mortality among high-titer vaccine recipients, and the results were presented at a second WHO-sponsored consultation in Atlanta on 16 and 17 June 1992. The consultative committee concluded that there was excess mortality associated with the high-titer vaccines. The committee recommended that no further studies of high-titer measles vaccines derived from the original Edmonston virus isolate be conducted in children and that the recommendation for the use of these high titer measles vaccines in immunization programs be rescinded.” [101]
The reason for that was because they believed the signal was clear enough that it would be unethical to risk any further deaths due to high titer vaccine.
It found that the standard-titre vaccine was simply more effective in reducing mortality rates, especially in girls
The results from Guinea-Bissau, Senegal and Haiti, all with high background child mortality, showed an association between high dose measles vaccines and decreased survival, especially among females, while studies from The Gambia and Mexico, where there was low background infant mortality, displayed no difference in mortality. This suggests that the medium and high titre vaccines do not cause excess mortality by themselves, and have been interpreted as evidence that any high dose vaccine attributable effect on mortality is multiplicative rather than additive.
Then why did Dr. Aaby state that if the vaccine was not pulled, it would have been disastrous with ½ million unnecessary deaths per year? Does it matter if it is ‘multiplicative or additive’ to the ½ million per year that would have died? And does anyone know if the depletion of vitamin A stores from high dose vaccines portends a worse outcome in those infants who live in places with high background mortality?
It has also been suggested that the impact of the vaccine may correspond to the delayed excess mortality reported after measles infection. However, even in areas with high mortality, medium and high titre vaccines were not associated with increased mortality between 5 and 10 months of age, when the standard group were still not immunized against measles. Since the difference is only found after the standard group have received SWS and in areas with high background mortality, the observed mortality differences may be attributable to beneficial effects of SWS vaccines, particularly for girls, which are not reproduced by the high titre vaccines.
In this context it is notable that studies in Bissau, Senegal and Haiti, have shown greater reductions in all cause mortality among recipients of standard measles vaccines, than could be explained by the prevention of acute measles deaths alone. In conclusion, there is no conclusive evidence that high titre vaccines are deleterious and it remains possible that they are just less beneficial than standard titre vaccines.
Again “Isabella B” is referred back to Dr. Aaby’s own statements that the vaccine could have led to a disaster, and ignores his subsequent finding that the CAUSE of the higher mortality was the use of the DPT vaccine as a “last” vaccine. Dr Aaby was not so cavalier about his facts, as “Isabella B” seems to be.
Her defense of the high titer vaccine is interesting, given that the part of the book under attack is about vitamin A supplementation to acutely infected children, and about the importance of nutrition.
“Isabella B” doth protest much over the quotes used, regarding the dangerous and abandoned high titer measles vaccines.
Conclusion
The number of important points missed by “Isabella B” is just as important as the misrepresentations.
Dissolving Illusions contains over 800 references many with direct quotes. The book also contains over 50 graphs and numerous photos. We have gone through a great deal of work to make sure that the information is accurate and honest. It was not whimsically put together but was years in the making and it was vetted by several medical professionals. And . . . as you can see, we were open to criticism even from a phantom committee hiding behind a fake name. It was a clever move to use a ‘mother’ as a front, since had the writers done such a blog under their real names they may have been constrained by the ethics committee on professionalism.
Only one criticism had any validity and that was changed nearly a year ago.
Any reader can read for themselves, the literature from the 1800s and 1900s. Dissolving Illusions provides the reader with direct information as well as a starting point for further research. There are certainly points that can be debated and expanded upon. No published work is perfect, but for the most part the criticisms put forward by “Isabella B” are neither accurate, nor well referenced, and clearly show both scientific ignorance and lack of objectivity.
Addendum: Authors’ analysis of “Isabella B’s” blog.
“Isabella B” claims to have started researching in 2014, and had enough of an interest in homeopathy to get Dissolving Illusions from a homeopath.
What mother who has just had a baby, reads a book, researches the whole book, then puts out three complex blogs, including the critique of Dissolving Illusions, in the space of three days? Then publishes another three blogs and drops the ball and runs?
It is doubtful whether this truly is a “crunchy” mother at all. Her “crunchy background” is posited as qualifying her ability to think, whereas Dr Humphries’ medical education counts for nothing. Having a crunchy background more accurately appears to simply appeal to the desired audience.
We welcome a second chance to educate readers as to the published facts of the matter, and trust that anyone who reads such a blog in the future will take close note of the weight of the arguments and the professionalism on either side.
References:
[1] Nicholson R “Measles and Deception. The epidemic that never was.” Bulletin of Medical Ethics, July/August, 1995, No.110., pp. 3-9.
[2] Aaby 2012 PMID 22700785
[3] BMJ 1959. Measles reports from general practitioners. Feb 7;1:380-383 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1992477/pdf/brmedj02957-0102.pdf?
[4] D. Griffin et al., “Measles Vaccines,” Frontiers in Bioscience, vol. 13, January 2008, pp. 1352–1370.
[5] http://www.ktuu.com/news/news/state-measles-test-on-alaska-girl-comes-back-negative/30969730
[6] http://www.ctvnews.ca/health/mystery-solved-northern-ontario-toddler-didn-t-have-measles-health-unit-says-1.2257693
[7] Aaby 2003 PMID: 12690020, Aaby 1996 PMID: 8684874, Aaby 1996 PMID 8629610, Aaby 2002. PMID: 12443670
[8] Koskiniemi 1997. Epidemiology of encephalitis in children. A prospective multicentre study. Eur J Pediatr 156: 541-545
[9] Roush 2007 PMID:18000199
[10] Sandford-Smith 1979 PMID: 508686
[11] Sauter 1982, PMID: 7179457
[12] Antonio C. Arrieta, MD; Margaret Zaleska, RN; Harris R. Stutman, MD; and Melvin I. Marks, MD, “Vitamin A Levels in Children with Measles in Long Beach, California,” The Journal of Pediatrics, July 1992, p.75.
[13] http://www.nzherald.co.nz/nz/news/article.cfm?c_id=1&objectid=9006061
[14] A. Langmuir, “The Importance of Measles as a Health Problem,” American Journal of Public Health, vol. 52, no. 2, 1962, pp. 1–4.
[15] Ibid.
[16] http://www.cdc.gov/vaccines/pubs/surv-manual/chpt07-measles.html
[17] Poland 2012 PMID 22196079.
[18] LeBaron CW, et al., “Persistence of measles antibodies after 2 doses of measles vaccine in a post-elimination environment,” Arch Pediatr Adolesc Med 161, 294-301 (2007). AND Heffernan JM, Keeling MJ, “Implication of vaccination and waning immunity,” Proc R. Soc. B 276, 2071-2080 (2009).
[19] http://query.nytimes.com/gst/abstract.html?res=9501E7D91430EE32A25757C1A96F9C946091D6CF
[20] http://www.nejm.org/doi/full/10.1056/NEJM196109142651101
[21] David J. Sencer, MD; H. Bruce Dull, MD; and Alexander D. Langmuir, MD, “Epidemiologic Basis for Eradication of Measles in 1967,” Public Health Reports, vol. 82, no. 3, March 1967, p. 256.
[22] Aaby 2003 PMID: 12505179
[23] Tobias 1987 PMID: 3451090, Leuridan PMID: 17629601, Papania 1999 PMID: 10545585
[24] Poland 2012 PMID 22196079
[25] CDC MMWR April 17, 2015
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6414a1.htm?s_cid=mm6414a1_e
[26] Murti 2013 PMID: 24330942
[27] http://www.ctvnews.ca/health/mystery-solved-northern-ontario-toddler-didn-t-have-measles-health-unit-says-1.2257693
[28] Singh 2002 PMID: 12145534, Singh 2003 PMID:12849883, Singh 2004 PMID:14729233, Singh 2009 PMID: 19758536
[29] Vijendra K. Singh, Ph.D. Congressional Testimony – April 6, 2000
[30] Paul Offit on radio 640AM with Thompson and Espinoza Jan 29, 2015 link: http://www.kfiam640.com/media/podcast-thompson-and-espinosa-thompsonespinosa/measles-outbreak-1pm-129-25774073/
[31] https://www.youtube.com/watch?v=dNwVf9LqwfI&list=PLgH2vCx5TOgXqctrxf-malkssiZajeo29 AND another video in Dr. Humphries possession.
[32] Kaic 2010 PMID: 20822734
[33] Murti 2013 PMID: 24330942
[34]http://www.hopkinsmedicine.org/kimmel_cancer_center/patient_information/Patient%20Guide%20Final.pdf
[35] Farrington 1995 PMID: 7619183
[36] Nieminen 1993 PMID: 8495082
[37] O’Leary 2012 PMID: 22232308
[38] Demicheli 2012 PMID: 22336803
[39] Koskiniemi 1989. EFFECT OF MEASLES, MUMPS, RUBELLA VACCINATION ON PATTERN OF ENCEPHALITIS IN CHILDREN. The Lancet Jan 7. pp. 31-34.
[40] Ibid Koskiniemi 1989.
[41] Koskiniemi 1997. Epidemiology of encephalitis in children. A prospective multicentre study. Eur J Pediatr 156: 541-545
[42] Ibid Koskiniemi 1997.
[43] A. Bitnun et al., “Measles Inclusion-Body Encephalitis Caused by the Vaccine Strain of Measles Virus,” Clinical Infectious Diseases, vol. 29, no. 4, October 1999, pp. 855–861.
[44] Dick G. Register of cases of subacute sclerosing panencephalitis. Br Med J 1973;3:359-60.
[45] Xu S. et al., 2013. “Genetic characterization of the hemagglutinin genes of wild-type measles virus circulating in China, 1993-2009.” Plos one. Sept. vol 8 issue 9. PMID: 24073194.
[46] http://data.worldbank.org/indicator/SH.IMM.MEAS/countries
[47] Finsterbusch 2009
[48] Klingele M et al., 2000. Resistance of Recent Measles Virus Wild-Type Isolates to Antibody-Mediated Neutralization by Vaccinees with Antibody. J Med Virology 62:91-98.
[49] Sanders R. Risk analysis for measles reintroduction post global certification of eradication. Geneva: World Health Organization; 2010. Available from: http://www.who.int/immunization/sage/7._Measles_post_eradication_risk_analysis.pdf
[50] Schrag A et al., 1999, “Spontaneous mutation rate of measles virus: direct estimation based on mutations conferring monoclonal antibody resistance.” J of Virology, Jan, p 51-54.
[51] Kweder A., 2014, “Mutations in the H,F, or M proteins can facilitate resistance of measles virus to neutralizing human anti- MV sera.” Adv in Virology, Feb 2014, pp 1-18 PMID: 24648840
[52] Shi et al., 2011. “Measles incidence rate and a phylogenetic study of contemporary genotype H1 measles strains in China: is an improved measles vaccine needed?” Virus Genes. 43:319-326. PMID: 21701857.
[53] Ibid Shi.
[54] Aaby 1995 PMID: 7502100
[55] Huiss, Damien et al., 1997. “Characteristics of asymptomatic secondary immune responses to measles virus in late convalescent donors.” Clin Exp Immunol 109:416-420. PMID: 9328115
[56] Ibid.
[57] Ibid.
[58] Damien et al., 1998. “Estimated susceptibility to asymptomatic secondary immune response against measles in late convalescent and vaccinated persons.” J of Med Virology. 56:85-90. PMID: 9700638.
[59] Federal Register. Vol 49, No 107. Friday Jun1 1984.
[60] Damien et al., 1998. “Estimated susceptibility to asymptomatic secondary immune response against measles in late convalescent and vaccinated persons.” J of Med Virology. 56:85-90. PMID: 9700638.
[61] Griffin D. et al., 2008. “Measles vaccines.” Frontiers in Bioscience 13, 1352-1370, January 1.
[62] “Measles as an Index of Immunological Function,” The Lancet, September 14, 1968, p. 611.
[63] A. Casadevall et al., “A Reappraisal of Humoral Immunity Based on Mechanisms of Antibody Mediated Protection Against Intracellular Pathogens,” Advances in Immunology, vol. 91, 2006, pp. 1–44.
[64] J. D. Cherry, “The ‘New’ Epidemiology of Measles and Rubella,” Hospital Practice, vol. 15, no. 7, July 1980, pp. 49–57.
[65] Ibid. Cherry.
[66] http://www.ktuu.com/news/news/state-measles-test-on-alaska-girl-comes-back-negative/30969730
[67] http://www.ctvnews.ca/health/mystery-solved-northern-ontario-toddler-didn-t-have-measles-health-unit-says-1.2257693
[68] Majumder 2015 PMID 25774618
[69] Murti 2013 PMID: 24330942
[70] http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/appendices/A/mmr_ig.pdf
[71] http://publichealth.lacounty.gov/ip/providers/Alert/Measles_Immune_Globulin_20140401.pdf
[72] http://www.cdph.ca.gov/HealthInfo/discond/Documents/CDPHIGforMeaslesPEP.pdf
[73] http://www.historyofvaccines.org/content/timelines/all
[74] Nicholson R “Measles and Deception. The epidemic that never was.” Bulletin of Medical Ethics, July/August, 1995, No.110. pp. 3-9.
[75] https://www.gov.uk/government/publications/measles-deaths-by-age-group-from-1980-to-2013-ons-data/measles-notifications-and-deaths-in-england-and-wales-1940-to-2013
[76] CDC measles complications http://www.cdc.gov/measles/about/complications.html last accessed 27th Sept 2015
[77] http://www.cdc.gov/vaccines/pubs/surv-manual/chpt07-measles.html
[78] Rønne. The Lancet, vol. 325, no. 8419, January1985, pp. 1–5.
[79] Uhlmann 2002 PMID:11950955
[80] S. J. Walker et al., “Persistent Ileal Measles Virus in a Large Cohort of Regressive Austistic Children with Ileocolitis and Lymphonodular Hyperplasia: A Revisitation of an Earlier Study,” International Meeting for Autism Research, Montreal, Canada, June 3, 2006.
[81] H. Kawashima et al., “Detection and Sequencing of Measles Virus from Peripheral Mononuclear Cells from Patients with Inflammatory Bowel Disease and Autism,” Digestive Diseases and Sciences, vol. 45, no. 4, April 2000, pp. 723–729.
[82] Poland 2011 PMID 22241978, Poland 2012 PMID: 22196079, Haralambieva and Poland 2013 PMID: 23256739
[83] Dhiman 2005 PMID: 16297162
[84] Poland 2012 PMID: 22196079
[85] Haralambieva 2013 PMID 23256739
[86] White 2012 PMID: 22230586
[87] Aaby 2011 PMID:21278492
[88] Aaby 2003 PMID: 12842371
[89] Sorup 2015 PMID: 25446818
[90] Aaby 2003 PMID: 12690020, Aaby 1996 PMID: 8684874, Aaby 1996 PMID 8629610, Aaby 2002. PMID: 12443670
[91] Aaby 1996 PMID: 8684874
[92] Aaby 1996 PMID 8629610
[93] Aaby 1995: PMID: 7502100
[94] Garly and Aaby PMID:12505179
[95] Oxford Textbook of Medicine, vol. 1, 2005, p. 357.
[96] (S. A. Silfverdal et al., “Breast-Feeding and a Subsequent Diagnosis of Measles,” Acta Paediatr, vol. 98, no. 4, April 2009, pp. 715–719.)
[97] Benn 2012 PMID:22239846
[98] S. Songül Yalçin, MD, and Kadriye Yurdakök, MD, “Sex-Specific Differences in Serum Vitamin A Values After Measles Immunization,” The Pediatric Infectious Disease Journal, 1999, p. 747.
[99] Yalçin SS et al. The effect of live measles vaccines on serum vitamin A levels in healthy children.PMID:9745778
[100] Aaby 2011 PMID:21278492
[101] Holt 1993 PMID: 8228340